Several clinical cases with lung sarcoidosis have been described. The article discusses the possibilities and difficulties of differential diagnosis. The interest in the cases described is that the disease was initially interpreted as pulmonary tuberculosis. And only after a histological examination of the biopsy material, the correct diagnosis was made.
Actuality.The issues of early diagnosis of granulomatous lung diseases remains an urgent problem, despite the widespread introduction of modern methods of radiation diagnosis, in particular, computed tomographic examination (CT) of the thoracic segment of the lung. This situation is due to the relative complexity of the differential diagnosis of sarcoidosis and pulmonary tuberculosis only on clinical grounds and data from visual research. In clinical practice, problems with nodular and disseminated forms of sarcoidosis and pulmonary tuberculosis often occur when determining the stage of the disease, assessing the dynamics of the process and its prognosis [1,2]. It is known that late diagnosis makes a prognosis
Patients with sarcoidosis of the lung are unfavorable, in particular at the stage of formation of irreversible fibrotic changes [3,4].
In this regard, the development of the algorithm and criteria for the clinical and morphological diagnosis of sarcoidosis and other granulomatous lung diseases is of particular relevance [5].
Methods.We present our own observations from practice related to the difficulties of differential diagnosis in sarcoid reactions, which may mask the clinical picture of the disease and are characterized by controversial manifestations in visual diagnosis, accompanied, as a rule, by misinterpretation of diagnostic signs. At the same time, morphological verification of a clinical diagnosis is of great diagnostic importance.
Clinical case 1.
Patient A., 46 years old, came to the pulmonary-surgical department of the Regional TB Dispensary with focal changes in the lungs, detected at the next routine examination.
It is known from ananesia that he considers himself a patient since March 2016, when, during the passage of fluorography, an increase in mediastinal lymph nodes was detected. An additional examination of the CT of the chest from 04.14.16 revealed a pattern of bilateral focal lesions, interstitial lung damage, and lymphadenopathy of the intrathoracic lymph nodes. Consulted by a phthisiologist, the results of bacteriological examination of sputum for Mycobacterium tuberculosis (3-fold) were negative, data for a specific process were not revealed. Recommended for the purpose of morphological verification of the diagnosis of lung biopsy. Surveyed on an outpatient basis. The patient was hospitalized as planned in the department of thoracic surgery. Overall condition is satisfactory. Conscious, adequate. Normostenic physique, satisfactory nutrition. Peripheral lymph nodes are not palpated. Osteo-articular system without visible deformities. Auscultation hard breathing, single dry rales, NPV 20 per min. The region of the heart is not visually altered. Auscultation heart sounds of sufficient sonority, regular rhythm. HR 80 per minute BP-120 and 80 mm Hg. Art. Biochemical blood test within normal limits. CT data from 04/14/16g. CT picture of bilateral focal changes, interstitial lung lesions, enlarged mediastinal lymph nodes, more data for sarcoidosis (tuberculosis?). Consultation of a phthisiologist of the Regional TB Dispensary on 04/19/16: consultation of a thoracic surgeon is recommended and the diagnosis is made: Sarcoidosis 2 tbsp. Disseminated pulmonary tuberculosis?
For the purpose of morphological verification of the diagnosis of 05/17/16, video assisted thoracoscopy (BATS), a biopsy of the right lung, was performed. The result of the histological study (at the first viewing of the microdrug), where the pathologist made the conclusion: "Dissemination of tuberculous etiology in the lung tissue." Data CT scan from 07.12.2016 the picture is typical for small and medium-focal pulmonary dissemination (more data for tuberculosis?). Consolidation of lung tissue in S l, 2 of both lungs, in S3 on the right, more data for pneumovirus. Increased intrathoracic lymph nodes. Pleural adhesions on both sides. It was consulted by a tuberculosis specialist, who concluded that given the clinic, the data for pulmonary tuberculosis are questionable, it was recommended prior to an outpatient examination. Discharged from the hospital in a satisfactory condition. Since the patient's condition deteriorated and the treatment did not give a positive effect, the histological material was sent for consultation to the Department of Pathological Anatomy of the Karaganda State Medical University, where microscopic samples of lung and lymph node were presented according to this observation in order to morphologically verify the clinical diagnosis.
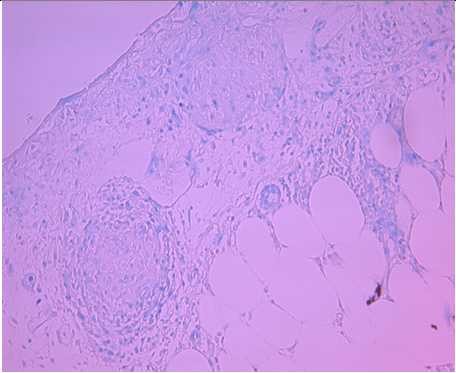 The result of repeated histological examination of microscopic preparations showed that the lung tissue was taken from the subpleural zone, where the formation of granulomatous structures is observed, in the giant cell granuloma stage with the formation of giant multinucleated cells of the Langhans type, the nuclei in them are arranged as a placer. Among them are lymphoid cells, granulomas are separated from each other by concentrically arranged fibers of coarse fibrous connective tissue tissue, the pleura is thickened due to sclerotic changes (Figure 1a, b).
The result of repeated histological examination of microscopic preparations showed that the lung tissue was taken from the subpleural zone, where the formation of granulomatous structures is observed, in the giant cell granuloma stage with the formation of giant multinucleated cells of the Langhans type, the nuclei in them are arranged as a placer. Among them are lymphoid cells, granulomas are separated from each other by concentrically arranged fibers of coarse fibrous connective tissue tissue, the pleura is thickened due to sclerotic changes (Figure 1a, b).
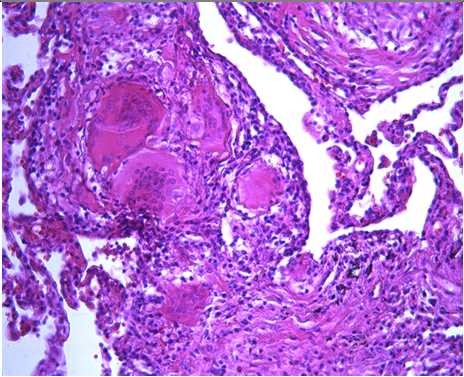


Figure 1 Lung sarcoidosis: a formation of giant cell granulomas, among them multinucleated cells; b sarcoid granulomas are surrounded by bundles of
connective tissue fibers. Staining: hematoxylin and eosin; c foci of atelectasis and compensatory emphysema in the PAS reaction; d Ziehl-Neelsen staining -
specific changes in the form of Mycobacterium tuberculosis were not detected
In other areas, the lung structure is preserved, there are foci of atelectasis and compensatory emphysema.
On the basis of microscopic data, it follows that the zone of caseous necrosis in the center of the forming granulomas is absent, which is not characteristic of the tuberculosis process, and the structure of granulomatous structures is not typical. When staging the histochemical reactions of the PAS reaction (Fig. 1c) and staining with Ziehl-Neelsen (Fig. 1d), no specific changes in the form of Mycobacterium tuberculosis were detected. The detected changes are the morphological equivalent characteristic of lung sarcoidosis, which served as the basis for the following conclusion: “Lung sarcoidosis at the stage of formation of giant cell granulomas”.
Case report 2.
Patient S., 48 years old, was admitted to hospital with a clinical diagnosis: Bronchiectasis in the upper lobes of both lungs, complicated by chronic inflammation, perifocal interstitial pulmonary fibrosis. Respiratory failure 0-1 degree.
Complaints at admission: low-intensity cough with the separation of a small amount of mucus mucus sputum, constant feeling of congestion in the chest, shortness of breath, expiratory character with moderate exertion, hoarseness, feeling of heat inthe back, general weakness. On examination, the general condition is relatively satisfactory, the skin is clean, the lymph nodes are not enlarged. Auscultatory harsh breathing, wheezing is not heard. For other organs without features. According to laboratory data, there was no change in the general analysis of blood and biochemical parameters. Microscopic examination of sputum for acid-resistant bacteria (CUB) from 04/25/2018 for Mycobacterium tuberculosis was three times negative. Spirograph on 04.24.2018 the function of external respiration is not impaired. The sample with bronchodilators is negative. CT scan of the chest without contrast dated April 23, 2018 showed the presence of bronchiectasis in the upper lobes of both lungs, mediastinal lymphadenopathy.
Histological examination of the sent material revealed lung tissue with intact histostructure. There are foci of compensatory emphysema with ruptures of the interalveolar septa, foci of atelectasis, hypertrophy of the muscle layer of arterial vessel walls of different caliber is noted, in some areas of the lung parenchyma lymphoid cell perivascular infiltration is observed. Blood vessels. Most of the bronchi and bronchioles are in a spasmed state, some with a scalloped lumen, hypertrophy of the muscular layer of their walls, peribronchial fibrosis is noted, in some areas moderate peribronchial lymphoid infiltration is noted. In the lumens of the bronchi and bronchioles desquamative exudate (Figure 2 a, b).
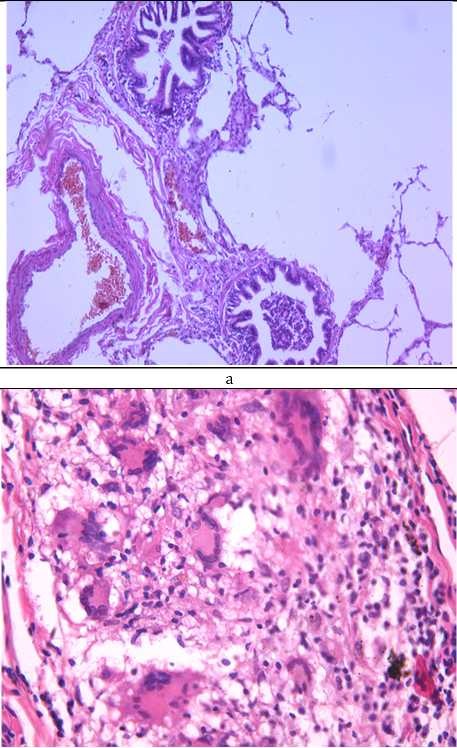

Figure 2 Granulomas in sarcoidosis. a-bronchial spasm. peribronchitis; b perivascular infiltrates; c giant cell granulomas
in sarcoidosis; d confluent granulomas. Staining: hematoxylin and eosine, b, d х 200; c х 400;
However, sometimes there are single granulomatous structures of small size, built of epithelioid cells, lymphocytes and among them groups of multicore cells with large hyperchromatic nuclei, some granulomatous structures germinate with connective tissue fibers. Granulomas are mainly localized in the subpleural zone and single in the lung parenchyma of minor size, mostly solitary, located perivascular, there are separate groups of small granulomas merging together (Fig. 2, c, d). The visceral pleura in areas of fibrosis is thickened, there are fields of fibrosis of the lung parenchyma and coils of angiosclerosis with obliteration of their lumen.
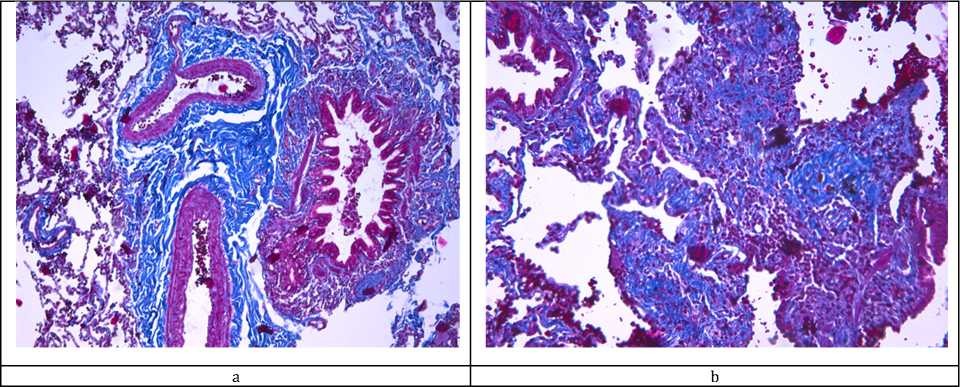
When Masson-Trichrome is stained to reveal the process of fibrosis, blue staining of the perivascular, peribronchial and subpleural zones is noted, and fibrosis is also found in the structure of the granulomas themselves (Figure 3 a, b).
Based on the morphological verification, the conclusion was made: “Epithelioid-lymphoid cell granulomas with giant cell transformation in sarcoidosis. Spastic obstructive bronchitis, bronchiolitis, peribronchitis. Secondary hypertrophy of arterial blood vessels. Subpleural fibrosis and focal pneumofibrosis ". Clinical case 3.
Figure 3 - Lung sarcoidosis. a - perivascular and peribronchial sclerosis; b - fibrosis in the area of granulomas. Staining Masson-Trichrome on the process of fibrosis а, b х 200;
Patient S., 61 years old, was admitted in 2016 with complaints of moderate chest pain to the left, in the area of the postoperative scar, a decrease in exercise tolerance. From the anamnesis of life, the patient was observed for several years about arterial hypertension with elevations of systolic blood pressure up to 200 mm Hg. Of the bad habits of smoking for 40 years, 2-1 packs per day. For 4 years he worked in hazardous conditions at a tannery. Regarding the identified, on the radiograph of the lungs, focal changes were examined in the tuberculosis clinic for tuberculosis and oncological process. The examination took place over 4 months, but the diagnosis was not established. Given the clinical symptoms, CT scan of the lung, a preliminary diagnosis of “Lung sarcoidosis” is made. He was directed to a video-assisted thoracoscopic lung biopsy for the purpose of morphological verification of the diagnosis. However, according to the results of the biopsy of 10/31/2016. granulomas with fibrinoid necrosis, giant Langhans cells were detected. Fully tuberculous process is not excluded. He applied for consultation to the pathological laboratory of the Karaganda State Medical University (Karaganda).
According to CT, signs of bilateral disseminated pulmonary lesions are predominantly in the upper lobes, similar to the picture of sarcoidosis.
With repeated histological examination in the sent material, lung tissue is represented by granulomatous structures, mainly characteristic of sarcoid granulomas in the formation stage of giant cell granulomas with fancy multicore cells like Langan's, the nuclei resemble a scattering of coins, are centralized.
Figure 4 Lung sarcoidosis. a granulomas in sarcoidosis with the formation of multinucleated giant cells, the nuclei of which are arranged randomly in the form of a “placer of coins” or “fingers of gloves”; b fibrinoid necrosis in the area of granulomas. Staining:
hematoxylin and eosin: а, bx 400;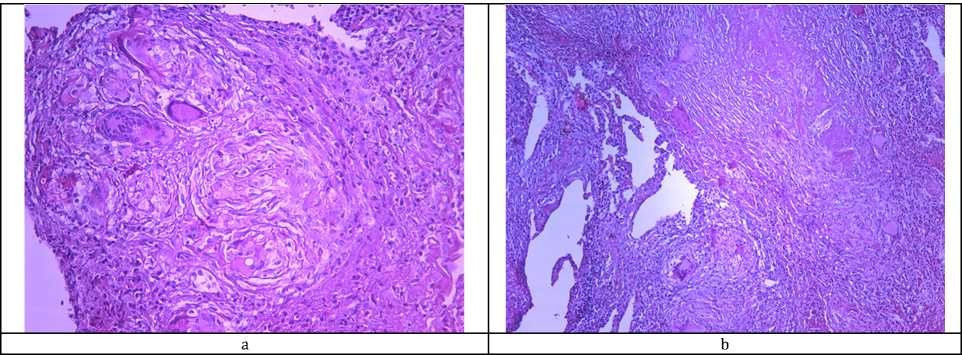
Granulomas are located compactly in the perivascular zone, consist of lymphocytes with the formation of lymphoid follicles without centers of reproduction. Granulomatous structures are located close to each other and are divided among themselves by bundles of coarse-fibrous connective tissue, a number of granulomas in the organization and hyalinosis stages. In some areas, fibrinoid necrosis was detected in the granuloma zone(Fig.4 a,b).
Based on the data of repeated microscopy, a conclusion was made: Sarcoidosis in the stage of giant cell granulomatosis with organization.
Conclusion.The presented clinical cases show the complexity of the clinical and morphological substantiation of granulomatous lesions, in particular in sarcoidosis and pulmonary tuberculosis, which is due to the lack of diagnostic criteria and practical experience of the pathomorphology. The complexity of the diagnosis of sarcoidosis is associated primarily with the polymorphism of the manifestations of the disease and the characteristics of the clinical and morphological forms.
In this regard, we propose morphological signs that are most typical for sarcoidosis of the lungs: the formation of lymphoid cell granulomas with the presence of multicore giant cells such as
Langhans, the absence of caseous necrosis in the center, in the final fibrosis of granulomas with a centered location of connective tissue fibers. Characterized by the formation of granulomas along the bronchovascular bundle, pulmonary veins, in the wall of the pulmonary arteries, in the interlobar, segmental and lobar pleura, along the lymphatic vessels, as well as the diagnostic significance of Schaumann and Khamazaki-Veseberg.
REFERENCES
- Ponomareva E.Yu. Difficulties of diagnosis in disseminated processes in the lungs // Klin. the medicine. 2013. V.91, №7. P. 61-64.
- Tusupbekova MM, Bakenova R.A., Stabaeva L.M. Features of the clinical-morphological picture of the diagnosis of sarcoidosis of the lungs: a description of the clinical case. 2008. 86 р.
- Chuchalin A.G. Diagnosis and treatment of sarcoidosis. Summary of federal clinical guidelines. Part II. Diagnosis, treatment, prognosis // Herald of the modern wedge. medicine. 2014. V.7, № 5. P. 7381.
- Common patterns and disease-related signatures in tuberculosis and sarcoidosis // Proc. Natl. Acad. Sci. USA. 2012. Vol.109, №20. P. 7853-7858.
- Bakenova R.A. Tusupbekova M.M. Nygyzbaeva R.Zh. Imanbaeva G.N. Certificate of State Registration of Rights to the Object of Copyright. 2018. 139 р.