SUMMARY
In this paper, the efficacy of the VD scheme use in patients with newly diagnosed multiple myeloma for the period 2012-2017, in the department of hemoblastoses of Kazakh Institute of oncology and radiology was evaluated. The effectiveness of treatment was assessed after 4-6 cycles of VD.
Objective: To evaluate the efficacy of the VD regimen (bortezomib + dexamethasone) in the first line of multiple myeloma therapy.
Methods. The study included 40 patients with newly diagnosed MM who received treatment according to the VD scheme in the department of hemoblastoses of of Kazakh Institute of oncology and radiology from 2012 to 2017. The median age was 59 years (40-81 years).
Results. Using the VD scheme in patients with newly diagnosed MM, the overall response rate was 75%. 40.6% of patients complete remission was achieved, in 16.6% of patients was very good partial remission, in 43.3% of patients - partial remission. Progression of the disease on the therapy background according to the VD scheme occurred in 25% of patients. The median time to achieve complete remission was 4 months. The overall survival of patients was 28 months. The transferability of treatment according to the VD scheme was satisfactory regardless of the age of the patients. Among the side effects anemia (42.5), peripheral neuropathy (35.5%), asthenic syndrome (25%), dyspepsia syndrome (22.5%) were observed.
The conclusion. The VD scheme has a manageable and predictable toxic profile, is effective and plays an important role in MM therapy as a first line, and leads to a significant increase in the overall survival of patients compared to treatment methods without the use of proteasome inhibitors.
Multiple myeloma (MM) is a malignant lymphoproliferative disease, characterized by bone marrow infiltration by plasma cells, the presence of monoclonal immunoglobulin in serum and / or urine, and osteolytic bone lesions. According to the WHO classification, multiple myeloma (MM) refers to peripheral B-cell lymphoid tumors [1]. The disease was first characterized in 1844 by S. Solly as softening of bones with bone marrow infiltration [2]. MM is the second most common among malignant hematologic processes after non-Hodgkin's lymphomas. The median survival rate for this pathology is 3 years with the use of standard chemotherapy and 4-5 years with high-dose chemotherapy with auto-transplantation of SGC (stem hemopoetic cells). In most patients, after Iline therapy the relapse is developed, and their lifespan does not exceed 5 years from the time of diagnosis [8]. Despite the long-term study of MM, a good understanding of the pathogenetic mechanisms of the onset and course of the disease, this nosology remains incurable.
Objective: To evaluate the efficacy of the VD regimen (bortezomib + dexamethasone) in the first line of multiple myeloma therapy.
Materials and methods: The medical history and outpatient cards of patients with newly diagnosed multiple myeloma (MM) II-III A and B stages by B. Durie and
S. Salmon who received VD “bortezomib + dexamethasone” therapy at the department of hemoblastosis of of Kazakh Institute of oncology and radiology from 2012 to 2017 were analyzed. The effectiveness of the VD scheme was evaluated in patients aged 40 to 81 years (median 59 years) of which 21 (52.5%) women, 19 (47,5%) men, respectively (Table 1).
Table 1. Characteristics of patients.
|
Number of patients |
40 |
|
Men (Male) |
19 (47,5%) |
|
Women |
21 (52,5%) |
|
Average age |
59 (40-81) |
|
II stage |
17 (42,5%) ~ |
|
III stage |
23 (57,5) |
|
Plasma cells in the bone marrow |
38,4 (от 15,2% до 51,8%) |
|
Primary patients |
40 ~ |
|
Osteodestruction |
25 (62,5) |
|
Anemia of mild to moderate severity |
17 (42,5) |
According to the protocol, all patients received from 4 to 8 cycles of PCT (primary chemotherapy) according to the VD scheme “bortezomib + dexamethasone” was administered intravenously 1.3 mg / m2 on 1, 4, 8, 11 days, dexamethasone 20 mg /m2 i.v in 1-2, 4-5, 8-9, 11-12 days of the course. The course is repeated every 21 days. The interval between courses is 10 days.
The effectiveness of treatment was assessed using the criteria of EBMT [9] (Table 2). Complete remission (CR) was established in the absence of monoclonal immunoglobulin in serum or urine, a decrease in the number of plasma cells in the bone marrow to a level of less than 5%, stable bone state and normal concentration of calcium in the blood serum.
Partial remission (PR) was defined as a decrease in serum M-protein concentration in excess of 50% and in urine more than 90%, stable bone status and normal serum calcium concentration.
Progression of the disease (relapse) was established at a 25% increase (or appearance) in the level of monoclonal immunoglobulin (in the serum - more than 10 g / l, in the urine - more than 200 mg / day), detection of new foci of destruction in the bones of the skeleton, occurrence of hypercalcemia.
Overall survival was defined as the time interval from the date of inclusion in the protocol of patients to death from any cause or until the date of the last visit of the patient.
Table 2. ECMT response criteria
|
CR. Complete remission |
Less than 5% of plasma cells of normal morphology in the punctate of the bone marrow, received no earlier than one month after the completion of the course of therapy and the absence of monoclonal Ig in the blood serum and / or urine. |
|
Close to CR |
100% reduction in M-protein, but detectable highly sensitive immunofluorescence methods. |
|
VGPR (very good partial remission). |
More than 90% decrease in paraprotein in serum or urine. |
|
PR |
≥50% decrease in serum immunoglobulin and / or> 90% decrease in Bence-Jones protein. |
|
MR. Minimal response |
≥25 a decrease in the level of monoclonal immunoglobulin in the serum, ≥50% of the Bence- Jones protein in the urine. |
|
Great response |
75% reduction of M-protein, 5% or less of plasma cells. |
|
Stabilization of the process |
Stabilization of the parameters of the disease (including the number and size of bone destruction), a moderate decrease in the level of monoclonal Ig in the serum and the Bence-Jones protein in urine, against at least 3 cycles of chemotherapy. |
|
Resistance |
No reduction in the serum of the monoclonal immunoglobulin or Bence-Jones protein in the urine. |
|
Progression of the disease |
The appearance of a monoclonal immunoglobulin, a 25% increase in its level, the appearance of new foci of destruction in the skeleton or plasmacytoma. |
Results and discussion: When using the VD scheme in patients with the newly diagnosed MM II-III A and B stage by B. Durie and S. Salmon a total response to therapy was obtained in 30 (75%) patients, of which 12 (40.6%) achieved complete remission of the disease, 5 (16.6%) had very good partial remission, 13 (43.3% ) had partial remission. In 10 (25%) patients, progression of the disease (in connection with the lack of effect on the VD scheme, a transition to the line of bortezomib-containing regimens of therapy was carried out). The average time to achieve complete remission was 4 months, and the average duration of remission was 12.6 months (Table 3).
Table 3. Results of application of the VD scheme in primary patients with multiple myeloma.
|
Criteria |
Therapy of 1st line |
|
General response to therapy |
30 (75%) |
|
Complete remission |
12 (40,6%) |
|
Very good partial remission |
5 (16,6%) |
|
Partial remission |
13 (43,3%) |
|
Months until the remission is complete |
4 months. |
|
The duration of remission (months) |
12,6 months |
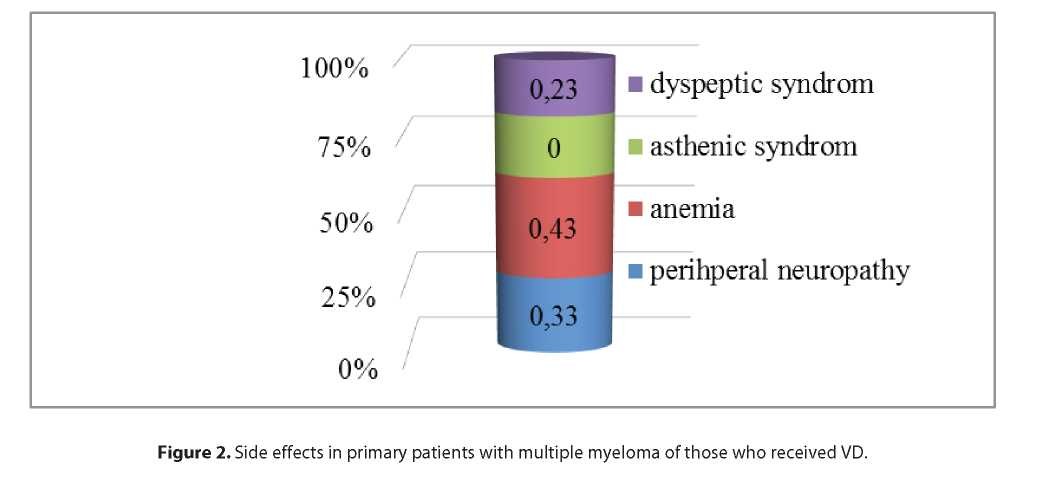
The use of the VD scheme in our study was accompanied by predictable and avoidable side effects. Among the side effects anemia (42.5), asthenic syndrome (25%), dyspeptic syndrome and peripheral neuropathy (35,5%) were observed.
Of the manifestations of non-hematological toxicity, the most frequently the peripheral neuropathy was observed. Peripheral neuropathy was reversible within 3-4 months after the appointment to patients with a long complex of B vitamins (neuromultivitis, milgamma), thioctic acid (thiogamma, thiocytide), anticonvulsants, with neuropathic pains (tebantin, pregabalin).
The asthenic syndrome was more often observed during the first three cycles of therapy. Most patients, despite the appearance of fatigue and weakness, could continue treatment.
Table 4. Side effects in primary patients with multiple
myeloma after VD.
|
Side effects |
Number of patients |
|
Peripheral Neuropathy |
13 (32,5%) |
|
Anemia |
16 (42,5%) |
|
Asthenic syndrome (fatigue, weakness) |
10 (25%) |
|
Dyspeptic Syndrome |
9 (22,5%) |
Anemia was observed in 16 (42,5%) patients. In patients who had reached the PR or the PR, the hemoglobin level increased. There was a parallel decrease in the need for transfusion of erythrocyte mass, and by the 5th cycle of treatment it was not required for any patient who achieved an objective response. Patients often had anemia of mild to moderate severity, which did not require blood transfusion therapy, was corrected by the appointment of erythropoietin. Also, 9 (22%) patients had dyspeptic syndrome.
Conclusion. The analysis of the obtained data shows high clinical efficacy and fairly good tolerability of bort- ezomib in combination with dexamethasone (VD scheme) as a program of choice in the first line of MM therapy.
Among patients who received bortezomib + dexamethasone, the total response rate was 75%. 40.6% of patients achieved complete remission, 16.6% of patients had very good partial remission, and 43.3% of patients had partial remission. Progression of the disease on the background

of therapy according to the VD scheme occurred in 25% of patients. The number of cycles of VD before receiving complete remission averaged 4 months. The overall survival of patients was 28 months.
Thus, the data obtained by us correlates with the results of international studies on the treatment of multiple myeloma. In particular, in the study of SS Bessmeltsev et al., the effectiveness of the VD scheme in 72 patients with newly diagnosed MM was evaluated. Several hematologic centers of the Russian Federation took part in this study [10]. The observation period for patients included in the study ranged from 3 to 49 months. GR (CR + PR), regardless of age, stage of disease and kidney function, was 54%, and taking into account the minimum response was 68%. In 12,5% of patients it was possible to receive CR and in 18% was almost CR. The PR was registered in 23.6% of patients. To obtain the CR, it took 5-8 cycles of VD. Partial remission or a minimal response was often observed after 3-4 cycles of therapy. During the first year, 98.6% of patients remained under observation, the second - 95.8%, and the third - 90.3%. Median OS (overall survival) in patients with CR and PR was not achieved, and in individuals with a minimal response it was 21 months. Thus, most MM patients responded to VD therapy. Analysis of survival of patients showed that the median OS at a follow-up period of up to 49 months. was not achieved. After reaching the answer, the patients were prescribed consolidation cycles, and subsequently they were transferred to the supportive therapy bort- ezomib + dexamethasone.
Data from large multicenter Phase II studies (SUMMIT (n = 193)) and Phase III (APEX (n = 669)) confirmed the high clinical efficacy of monotherapies with bortezomib in the treatment of patients with refractory / relapsing forms of MM. The general response (GR) to therapy with bortezomib was 43%, complete remission (CR) was 6%. Median OS was 29.8 months. [11, 12]. Even more effective was the use of bortezomib in combination therapy, in particular in combination with Dexamethasone, (the overall clinical response with this combination was more than 80%, complete remission (PR) - (40%), and median OS was 23.7%) [9, 10].
Thus, the VD scheme is an effective method of treatment in patients with the newly identified MM. This scheme allows to achieve a complete response in most patients with MM.
REFERENCE
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) Multiple Myeloma. www.nccn.org
- Rukavitsyn OA Hematology. National leadership. 2015. 565-573 p, 751.
- Volkova MA Clinical oncohematology: Hand-in for doctors. - M.: Medicine, 2007. - 1120 p.: ill.
- Kropff M.H., Bisping G., Wenning D.et al. Bortezomib in combination with dexamethasone for relapsed multiple myeloma. LeukRes 2011; 29:587—90.
- Jagannath S., Durie B.G.M., Wolf L.J. et al. Longterm follow-up of patients treated with bortezomib alone and combination with dexamethasone as frontline therapy for multiple myeloma. Blood. - 2013. - № 108 (11). - P. 796.
- Poddubnaya IV, prof. Savchenko VG, Russian Clinical Recommendations for the Diagnosis and Treatment of Lymphoproliferative Diseases, Moscow, 2016.
- Kaidarova D.R. et al. Indicators of Oncology Service of the Republic of Kazakhstan for 2015.
- Bessmeltsev SS, Abdulkadyrov KM. Multiple myeloma. A modern view of the problem. Almaty, 2007. 480 p.
- Blade J., Samson D., Reece D. et al. Criteria for evaluating disease response and progression in patients with multiple myeloma treated by high-dose therapy and haemopoietic stem cell transplantation. Br J Haematol 2013; 102:1115—23.
- Bessmeltsev SS, Stelmashenko LV, Karyagina EV New approaches to the treatment of multiple myeloma. Vestn. Ros. military-med. acad. 2010; 3: 149-54.
- Richardson P.G., Barlogie B., Berenson J. et al. A phase 2 study of bortezomib in relapsed, refractory myeloma // N. Engl. J. Med. 2003. 348. 2609– 2617
- Richardson P.G., Sonneveld P., Schuster M.W. et al. Bortezomib or high-dose dexametesone for multiple myeloma // N. Engl. J. Med. 2005. 352. 2487–98.
- Kropff M.H., Bisping G., Wenning D. et al. Bortezomib in combination with dexametasone for relapsed multiple myeloma // Leuk. Res. 2005. 29. 587–90.
- Popat R., Oakervee H., Williams C. et al. Bortezomib, low-dose intravenous melphalan and dexametasone for patients with relapsed multiple myeloma // Haematologica. 2008. 93. Abstract 918.