SUMMARY
Involvement in the pathological process of the cardiovascular system is described for all types of MPS.To conduct a study of the aortic root in children with MPS typesl, II, IVA and VLTransthoracic echocardiography assessment of the morphology of the heart and great arteries.Results:Among the children we observed, there were 8 children with MPS I type (25 %), 14 boys with MPS type Il (43.7 %), 4 children with MPS type IVA (12.5 %) and 6 children with MPS type Vl (18.7 %). According to the data of the echocardiogram, the mean value of the aortic root was 16.7±6.4 mm. The significant dilation of the aortic valve (z-score 3.0 and 3.6) and especially the Valsalva sinus (z-score 3.2 and 4.3) is a specific feature in both clinical cases. With a careful examination of the sinus Valsalva morphology in the first patient, we found an aneurysm of the right coronary sinus, which is a rare congenital pathology. In the second patient, the sinus of Valsalva was significantly enlarged, but without an aneurysmal component. Mild aortic regurgitation with Doppler echocardiography (PHT 720 msec) was registered in-patient M. In-patient P., regurgitation was moderate, which was indicated by the PHT index of 460 msec. In addition, the peak pressure gradient on the aortic valve was 27.8 mm Hg, indicating a mild stenotic component. We note a low incidence of aortic root damage in children with MPS in the Republic of Kazakhstan. However, it is necessary to take into account the international experience of maintaining this category of patients and the extreme unpredictability of the course of an aneurysm of the sinus of Valsalva in conditions of accumulation disease.
Mucopolysaccharidosis (MPS) is a lysosomal accumulation disease caused by impaired glycosaminoglycan metabolism (GAG) because of genetic inferiority of lysosomes enzymes participating in their cleavage [I].
Involvement in the pathological process of the cardiovascular system is described for all types of MPS. The aortopathyas dilatation with a significant decrease in elasticity has been described with MPS I type Scheie [2]. In patients with MPS I type, Hurler under 1-year-old, dilated aortic root was detected in 38 % [3]. The results of observations of 34 patients with MPS type I-VII, established dilatation of the aortic root in 35 % [4]. As a result of dilatation of the aortic root is an aneurysm followed by dissection and a high risk of death [5,6].
Objective: to conduct a study of the root of the aorta in children with MPS II, IVA, VI types and I.
Materials: 32 children with MPS types I, II, ΓVA and VI.
Methods: Echocardiography assessment of the morphology of the heart and great arteries. The examination was carried out with expert ultrasound InachincsToshibaArtida, and Philips E33. Evaluation of morphological structures was carried out in B and М-mode. The measurements were in accordance with the guidelines and recommendations of the European Society of Cardiovascular Imaging and the American Association of Echocardiography [7, 8].
The main positions for assessing the aorta were parasternal in the long axis of the left ventricle, parasternal short axis of the left ventricle at the level of the aortic root, the apical five-chamber view and suprasternal view. Measurements of aortic root diameter, sinus of Valsalva, and sinotubular junction were performed in В-mode in parasternal long axis view. Indexation of the indices was carried out in calculating the surface area of the body according to the Dubois formula[9].
Doppler echocardiographic evaluation of regurgitation was performed according to the recommendations of the European Association of Echocardiography in the case of PHT (pressurehalf-time), because due to the underlying disease it was difficult to exclude the pathology of the min,al valve. And also poor quality of visualization did not allow to carry out measurements by the PISA method (proximal isovelocity surface area). So, we carried out a measurement by linearly routing the continuum-wave Doppler contour of the regurgitation flow to the aortic valve and calculations of the mean values between the highest and lowest values of the flow velocity.
Results: Among the children we observed, there were 8 children with MPS I type (25%), 14 boys with MPS type II (43.7%), 4 children with MPS type IVA (12.5%) and 6 children with MPS type VI (18.7 %). The gender distribution was predominantly boys in the number of 23 (71.8 %), girls were 9 (28 %). The mean age at the time of the study was 8.4 years ± 5.3, from a minimum of 1 year to a maximum of 27 years. According to the data of the echocardiogram, the mean value of the aortic root was 16.7±6.4 mm. Based on the results of Echo in the study of the aortic root, our attention was drawn to the emphasis and severity of the sinus of Valsalva in two patients with MPS type II.
Patient M. with MPS type II,4 years old, the diagnosis of MPS was exposed on the basis of enzymodiagnostics and molecular genetic research at the age of 4 years. Complaints at the time of admission: delay in psycho-speech development, frequent respiratory infections, difficult and noisy nasal breathing. At the time of hospitalization, the condition of the child is difficult, due to the underlying disease, a backwardness in mental development. There was a lag in physical development, height 87 cm (on a centile scale below 3 percentile), weight 14 kg. (10 percentile), BSA 0.59 m2. Typical for MP Smoiphophenotype, with osteoar- ticular changes. Cardiovascular system: the heart region is visually deformed due to the underlying disease as a keeled thorax. Heart push is not strengthened. Percussion of the boundaries of relative cardiac dullness are enlarged due to the left heart (2.5 cm outside of the median-clavicular line on the left). Auscultation: heart sounds are muffled, a systolic murmur 2 of 6 is heard on the gradation of the murmur intensity of Freeman- Levine.
Second patient R. with MPS type II, 27 years old, the diagnosis of MPS was exposed on the basis of enzyme diagnosis and molecular genetic research at the age of 25 years. The patient complained of low stature, rough features. At the time of examination, the patient's condition is of moderate severity, due to the underlying disease. There was a lag in height - 147cm, weight 68 kg, BSA 1.15m2. Typical for MPS morphophenotype with Osteoarticular deformities. Cardiovascular system: the heart region is not visually defoιmed; the cardiac impulse is localized. Percussion: the boundaries of relative cardiac dullness are enlarged due to the left heart (2.0 cm to the outside of the median-clavicular line on the left). Auscultation: heart sounds are muffled, a systolic murmur 2 of 6 is heard on the gradation of the murmur intensity of Freeman-Levine.
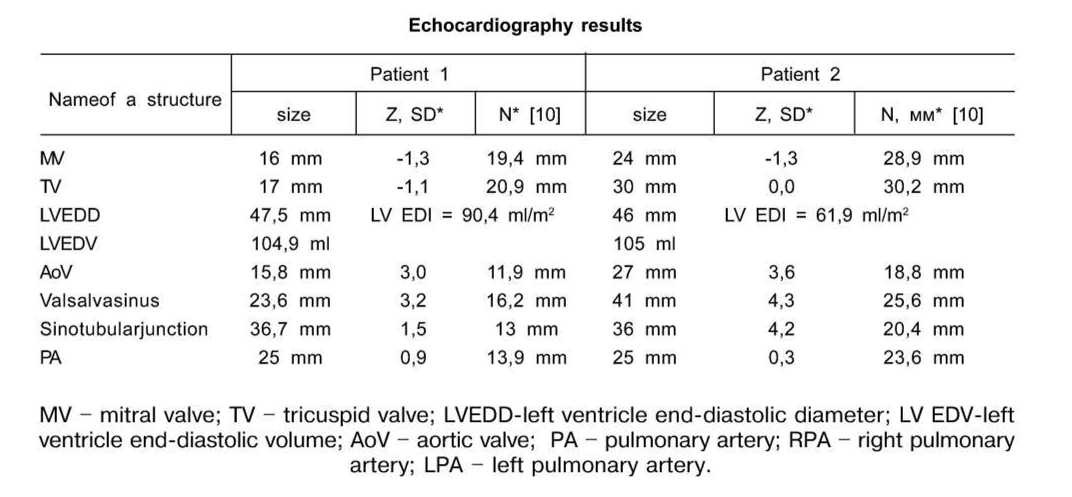
Both patients underwent a transthoracic echocardiography, the results of which are set out in table.
Wlien interpreting the data in patient No. 1, there was a slight decreasingof the size of the anioventricular valves. In this case, the indexed dimensions of the left ventricle in diastole indicate an expansion of the cavity (EDI 90ml / m2). Along with this, in the second patient the left ventricle volume was not expanded (EDI 61.9 ml / m2). Tlie significant dilation of the aortic valve (z-score 3.0 and 3.6) and especially the Valsalva sinus (z- score 3.2 and 4.3) is a specific feature in both clinical cases. With a careful examination of the sinus Valsalva morphology in the first patient, we found an aneurysm of the right coronary sinus, which is a rare congenital pathology. In the patient M. this morphology is also associated with the rare accumulation disease, which in turn makes the prognosis of the functional worsening of the aortic valve. In the second patient, the sinus of Valsalva was significantly enlarged, but without an aneurysmal component. That is, in the second child, the dilation of the sinus of Valsalva was a secondary genesis due to the underlying disease of accumulation.
The cusps of the aortic valve in both cases are insignificantly thickened. Insufficiency of the valve function was manifested by mild regurgitation with Doppler echocardiography (PHT 720 msec) in patient M. In patient P., regurgitation was moderate, which was indicated by the PHT index of 460 msec. In addition, the peak pressure gradient on the aortic valve was 27.8 mm Hg, indicating amild stenotic component.
In accordance with the functional classification of aortic regurgitation, wc regarded these cases as type 1, since the z-score of the aortic valve was 3.0.
According to the results of echocardiographic study, the patient M. has left ventricle hypertrophy - the relative thickness of the walls is 0.46 (the norm is 0.42). Myocardial mass index was 173.2. Along with this, the parameters of the second patient differ in isolated LV posterior wall hypertrophy (17 mm).
The function of the left ventricle is preserved: the ejection fraction in the patient M. and patient P. was 74.7% and 66.1%, respectively. The cardiac index is 4.7 I∕min∕m2 and 4.3 l∕min∕m2 without calculating the error for aortic insufficiency. Patient P showed a small accumulation of fluid in the pericardial cavity locally along the back wall of the LV The zone of dissynchronization and hypokinesia of myocardium of the left ventricle is also not recorded.
Conclusion: Despite the relatively high aortic dilatation rate according to the literature [3,4], the results of our observations revealed this pathology in only two patients out of 32, which was 6.25%. An aneurysm of the sinus of Valsalva is a rare congenital pathology (incidence 0.09%) [10], in which the right coronary sinus is most often affected, which is observed in patient M. This clinical case is even more rare, since there is a combination of two rare conditions: Iysosomes accumulation disease, which in its pathophysiology also affects the valves of the heart, and the aneurysm of the right coronary sinus of the aortic root without signs of rupture. We note a low incidence of aortic root damage in children with MPS in the Republic of Kazakhstan. However, it is necessary to take into account the international experience of maintaining this category of patients and the extreme unpredictability of the course of an aneurysm of the sinus of Valsalva in conditions of accumulation disease.
REFERENCES
- Atul Mehta, Bryan Winchester. Lysosomal storage disorders. A practical guide. Wiley-Blackwell, 2012. - 208 p.
- Elizabeth A.Braunlin, Paul R.Harmatz, Manrizio Scarpa, Beatriz Furlanetto, Christoph Kampmann, James P.Loehr, Katherine PPonder, William C.Roberts, Howard M.Rosenfe!d, Roberto Giugliani. Cardiac diseases in patients with mucopolysaccharidoses: presentation, diagnosis and managcment // Journal OfInherited Metabolic diseases, 2011.Dec; 34(6): 1183-1197.Published online 2011 Jul 9.doi: 10.1007/s 10545-011-9359-8
- Schroeder, L.; Orchard, P; Whitley, C.B.; Berry, J.; Tolar, J.; Miller, W.; Braunlin, E.A. Cardiac ultrasound findings in infants with severe (Hurler phenotype) untreated mucopolysaccharidosis (MPS) Type I // J. Inlierit. Metab. Dis. Rep. 2013; 10, 87-94.
- Meena Bolourchi, Pierangelo Renella, Raymond У Wang. Aortic Root Dilatation in Mucopolysaccharidosis I-VII // Int. J. Mol. Sci. 2016, 17, 2004. doi:10.3390/ijmsl7122004.
- Fikar, C.R.; Fikar, R. Aortic dissection in childhood and adolescence: An analysis of occurrences over a 10-year interval in New York State // Clin. Cardiol. - 2009. - Vol. 32. E23-E26.
- Shamszad, P; Barnes, J.N.; Morris, S.A. Aortic dissection in hospitalized children and young adults: A multi-institutional study // Congenit. Heart Dis. - 2014. - № 9. - P. 54-62.
- ACC∕AAP∕AHA∕ASE∕HRS∕SCAI∕SCCT∕SCMR∕SOPE2014 Appropriate Use Criteria for Initial Transthoracic Echocardiography in Outpatient Pediatric Cardiology, 2014 http://dx.doi.org/10.1016/ j.jacc.2014.08.003
- European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 1: aortic and pulmonary regurgitation (native valve disease) Patrizio Lancellotti (Chair), Christophe Tribouilloy, Andreas Hagendorff, Luis Moura, Bogdan A. Popescu, Eustachio Agricola, Jean- Luc Monin, Luc A. Pierard, Luigi Badano, and Jose L. Zamoranoon behalf of the European Association of Echocardiography. Document Reviewers: Rosa Sicari, Alec Vahanian, and Jos R.T.C. // Roelandt. Ernopean Journal of Echocardiography. - 2010. - № 11. - P. 223-244 doiH0.1093∕ejechocard∕jeq030
- Pettersen M.D., Du W., Skeens M.E., Httmes R.A. Regressione quations for calculation of z- scoresof cardiacstructures in a large Cohortofhealthyinfants, children and adolescents: anechocardio- graphic study // J. AmSocEchocadiogr. - 2008. - Vol.21. - P. 934-992.
- Sinus of Valsalva Aneurysms: Review of the Iiteratme and an Update on Management Michael Weimeich, MD, MPH; Pey-Jen Yu, MD; BianaTrost, MD Department of Medicine (Weimeich), Department of Cardiovascular Surgeiy (Yu), and Department of Cardiology (Trost), North Shore-Long Island Jewish Health System/Hofstra University School of Medicine, Manhasset, New York // Clinical Cardiology. - 2015. - Vol. 38, Iss. 3. - P. 185-189.