Abstract
Object: The socio-economic status of households with disabled children is the subject of worldwide attention for scientists and public policy. Such households suffer from a high probability of a social risk, which is generated by economic and social environment factors. The study aims to identify factors affecting the welfare of a family with child limitations, such as “mental retardation” and to assess the impact of each group of factors.
Methods: Authors applied the method of a sociological survey in five regions of Kazakhstan. The interview used a methodological approach based on identification of four types of restrictions: Direct costs for a child, indirect household losses, assessment of the possibility for a parent to find employment and maintain their health. The survey results were processed by PLS3-PM structural modeling, for which we accepted four types of constraints as dependent variables.
Findings: The econometric model allowed us to prove hypotheses regarding the degree of impact of restriction factors on the welfare of households with disabled children. To the greatest extent, the welfare of the family is limited by direct out-of-pocket expenses on the child’s needs. A significant value is the allowances associated with disability as the most important source of income. Statistically, insufficient volumes of medical and special social services increase direct costs considerably. An increase in the costs for a child is a prerequisite for reducing the family’s disposable income and its poverty.
Conclusions: The birth of a disabled child negatively affects the employment opportunities of at least one family member, their health, and development of human capital. Besides the loss of a parent’s income, indirect losses of a family have a significant prolonged effect on its long-term wellbeing as there is no affordable system for bringing a child into independent life in Kazakhstan.
The problem of disability in the modern world is acute. According to the World Health Organization, almost 15% of the world’s population has some form of disability, and the number is growing (WHO, World report on disability, 2012). Among them, 110 million (2.2%) to 190 million (3.8%) adults face serious life support difficulties every day. There are a lot of reasons for this: aging of the population, poor medical diagnostics at an early age and during intrauterine development, unavailability of modern health services, deterioration of the environmental situation, etc. (WHO, Disability and health, 2020).
Against the background of the general increase in the number of people with disabilities, child disability is also growing. That being said, both qualitative and quantitative assessment of child disability may sometimes be difficult. This is because each country keeps record of disabled children according to its own methodology, which sometimes makes it difficult to compare countries by the total number of children and the structure of specific diseases (Children with Disabilities // The state of the world’s children
*Responsible author:
E-mail address: dina131111@mail.ru
2013.). Statistics from many countries show an increase in the overall indicator. For example, Germany saw an increase of 3.7% over the period of 2015—2019 (https://www-genesis.destatis.de, 2021). Approximately the same situation is in Sweden, where the number of disabled children has increased by 1.2% (Försäkringskassan, 2021). In the UK, from 2011 to 2019, the number of children with mild, moderate and severe health disorders increased by 1.9% (https://www.ons.gov.uk, 2021). Despite the advances in medicine, child disability in highly developed countries does not weaken.
It is even more relevant for developing countries. For instance, in Russia over the past 5 years, the number of disabled children has increased by 9.2% (https://sfri.ru, 2021); in Moldova, the number of disabled children has grown by 1.1% (https://statbank.statistica.md); and 2.01% in Mexico (https://www.inegi.org.mx). The Republic of Kazakhstan can also be attributed to countries where the problem of child disability is very relevant. Today, 680 thousand people with disabilities live in Kazakhstan. Of these, 91.5 thousand are children with disabilities (https://bala.stat.gov.kz) and the number is constantly growing. The average annual growth rate is about 4.6% per year.
This is especially true for children with “mental retardation” (MR), a fairly large group united by the pedagogical criterion of restrictions in child learning.
According to O. A. Sergeyeva et al. (Sergeeva O.A., Filippova N.V., Barylnik YU.B., 2015) as of 2015, 25% of the child population suffers from MR. A.V. Goloshchapov (Goloshchapov A.V., 2015) cites data that about 20% of children at the time of admission to school have mental retardation, and about 50% of all children are not able to sufficiently follow the school curriculum. Most European and American sources indicate MR is taking up to 1–3% of the child population (Lukemeyer A. et al. 2000; Zaidi A, Burchardt T., 2005; Stabile M., Allin S., 2012; Okon M. et al., 2019; Morris Z., Zaidi A., 2020;). Mental retardation is currently one of the most common forms of child disability. However, most researchers agree that MR still has no clear definition (Pevzner M.S., 1972; Kovalev V.V., 1979; Kobernik G.I. Sinev. V. N., 1984; Lebedinskiy V., 2003; Lebedinskaya K.S.,2006; Emelina D.A., Makarov I.V., 2018).
As part of our study, we consider a large group of families with children sharing a diagnosis of MR, who have one or more signs (speech disorders, signs of autism, intellectual disabilities, mental disorders, etc.), that is, some commonality in the type of disability.
Initially, scientific research on the problem of child disability would be performed in pedagogy and medicine. For the first case, the family would be considered as the basis for raising a child with a disability; for the second case, as one of the important tools for rehabilitation and treatment of a disability. For a long time, it was believed that the state would do better. Some works (Vlasova T.A., Lebedinskaya K.S., 1975; Elfimova N.V., 1978) would suggest that for the successful treatment, rehabilitation and habilita- tion, a disabled child must be placed in specialized institutions where such children can receive the maximum number of services of an appropriate quality. With the development of humanistic processes in society, scientific papers substantiated methods of effective rehabilitation and habilitation of a child in the family (Ejdemiller E.G., 2008; Tkacheva V.V., 2014). There were studies that focused on social relations within the family in connection with the birth of a disabled child. (Muzaparova L.M., 2003). Today, most studies in developing countries consider medical or socio-psychological aspects in such families, e.g., L.M. Muzaparova, F. Baiserkina et al. who analyze the subject area of social issues and rehabilitation opportunities within the family (Bajserkina F., 2013).
Since the 90s, many scientists and charitable foundations have proved that the birth of a disabled child affects the well-being of the family since a significant number of restrictions arise. Problems appear in all spheres of family life with no exception: a psycho-emotional situation, relationships of family members, personal growth, public opinion, financial welfare, etc. Families regularly face a number of problems with consequences for the entire social group “family” and each of the people it includes (Carissa A. et al., 2009; UNICEF, May 2013; Giulio P. et al., 2014).
The state recognizes additional risks for such families at the level of official social policy through enhanced measures of their social support. Three main support measures on which family policy is based, according to standards recognized in developed countries, are family allowances, childcare services and kindergartens (daycare centers), and schools with an inclusive education model upon reaching school age. In the case of people with disabilities, they are transformed into an extensive range of additional allowances and services that provide full-fledged life activity for a child with special needs (ILO, 2004).
Economic issues of life support for disabled children involve a combination of various kinds of allowances in cash, tax benefits, and in-kind transfers, including in the form of services. The latter can address the issues of households with children, provide some services free. This is especially relevant, because many studies confirm that the costs of raising a special needs child are two to three times higher than the costs associated with children without disabilities (Langerman C., Worrall E., 2005; Kirton, D.2009).
For example, a number of researchers consider the problem of families with disabled children from an economic point of view: how does the birth and raising of such a child affect the structure of income and expenses, the parental employment, their professional growth, etc. According to researchers, the birth of a disabled child creates an additional burden (adds financial stressors to households) on the family budget. Also, the birth of a special needs child negatively affects the parental employment. The results of scientific research have shown that about 15% of parents (one of the parents) have completely ceased their work activities due to the birth of a disabled child, and about 17.4% have changed their jobs in order to get more opportunities to care for the child. Many studies have revealed that mothers mostly change their jobs or quit the labor market for good.
Ultimately, the financial burden on the family increases with the birth of a disabled child, which further pushes the household into poverty. After all, a special needs child requires additional costs: To be it medical, psychological, educational, or other rehabilitation services (direct financial costs), potential family losses due to a change in the status of parents (indirect costs). All this, according to the researchers, leads to a decrease in the financial stability of the household and will affect the further development of the family.
According to the literature review, many researchers have chosen a separate group of constraint factors for their papers. We can say that a comprehensive study of the group of restrictions and the degree of their impact on families with disabled children is not enough today. A whole number of researchers, such as LeaAnne DeRigne and Shirley L., state that as well (LeaAnne DeRigne, Shirley L., Porterfield, 2015).
In general, international practices of studying the factors of restrictions of households with disabled children are based on the study of three large groups of these factors:
- Direct costs factor, which includes the costs of a family to purchase necessary goods and services for a disabled child. Such expenses imply the actual costs incurred by the family as part of the life of a special needs child;
- Additional costs for goods and services. This group involves calculating additional costs for goods and services necessary for disabled children, but yet unavailable for various reasons. Such goods and services are necessary for certain activities they currently are not engaged in due to their disability.
- Cost equivalence. When using this method, the focus of study is various costs that a disabled person must incur so that they could enjoy the same quality of life as that with no disability (Zaidi A., Burchardt T., 2005; Stapleton D., Protik A., Stone C., 2008).
Thus, the birth of a child with a disability sets several restrictions on the development of the family is absolutely indisputable. Now, which of these restrictions have the greatest impact on the family, and which are less, and how are they interconnected?
The novelty of our research lies in the fact that based on the world research practices of studying families with disabilities we have developed a methodology adapted to Kazakhstan conditions for determining the impact of restriction factors on the welfare of a family raising a special needs child. We propose identification of four indicators reflecting the specifics of the well-being of a family with disabilities:
- Direct costs for a disabled child. These are influenced by a fairly large group of factors that lie on the side of the family characteristics, its expenses in connection with a child’s special needs. Direct out-ofpocket costs are due to family income and state allowances available to them.
- Indirect family losses associated with a reduction in income from employment of a family member who is constantly caring for a child and the need for services that arose due to the birth of a disabled child (short and long-term social respite).
- The parent’s ability to stay healthy.
- The parent’s opportunity to work.
Based on the analysis of the results of the survey and interviews, we have determined the degree of impact of each factor group on the welfare of a family with disabilities.
The purpose of the paper was to study the factors influencing the welfare of families with disabilities or raising children with delayed psychological development.
Experimental
We applied the method of sociological research and mathematical processing of its results using the PLS3-PM model.
The main method of collecting information was an interview; some questions were closed, and some were open. For the objects of the study, we have selected families raising children with MR as one of the most common types of restrictions. A total of 301 families took part in the survey. To ensure the representativeness of the sample, we have selected families from both urban and rural areas in four regions of Kazakhstan and Almaty. This allowed us to consider the specifics of the family’s place of residence.
We have formed an information base for creating the sample with the data provided by the Departments of Education of the Karaganda, East Kazakhstan, Pavlodar and Almaty regions, as well as the offices of psychological and pedagogical correction of the cities of Almaty, Karaganda, Pavlodar, Ust- Kamenogorsk, and Semey.
We shall present the structure of the closed part of the interview in more detail in the Results section.
The main purpose of the open part of the interview was to obtain data on the family’s life position, to let respondents express their private opinions on the rehabilitation system for the child, family members’ jobs, etc.
We used SmartPLS software to process the survey data. Using a graphical user interface, it simulates structural equations based on variance using the method of partial least squares modeling. In addition to evaluating models with latent variables using the PLS-SEM algorithm, the software calculates standard criteria for evaluating results. Thus, based on the results of mathematical modeling, we could determine the degree of impact of each of the restriction factors that negatively affect the indicators of the welfare of a family with a disabled child, including the nature of the relationship between dependent variables.
The mathematical model is based on a number of independent (Xn, the factors) and dependent variables (Ym, the indicators of well-being). To introduce both independent and dependent variables into the model, we have operationalized them using a 5-point scale, which allowed further econometric modeling (Table 1).
Table 1. Questionnaire structure and PLS3-PM model legend
|
Blocks |
Ref. |
Block components |
Ref. |
|
|
1 |
2 |
3 |
4 |
5 |
|
Indicators of well-being, Ym |
||||
|
1 |
The ability to stay healthy |
Y1 |
Counselling |
Y13health |
|
General healthcare |
Y14health |
|||
|
Medical procedures |
Y15health |
|||
|
2 |
Opportunity to work |
Y2 |
Full-time job |
Y10oppwork |
|
Part-time job |
Y11oppwork |
|||
|
The ability to work as a self-employed |
Y12oppwork |
|||
|
3 |
Indirect losses |
Y3 |
One of the parents is staying indoors and is unable to maintain full-time employment |
Y7indlos |
|
Paid healthcare/counselling for parents that are necessary due to the burden on the family |
Y8indlos |
|||
|
Paid services of “long respite” (vacation and treatment) |
Y9indlos |
|||
|
4 |
Direct out-of-pocket expenses for a child, in % of average monthly income |
Y4 |
Total costs |
Y1dcosts |
|
Medical facilities and care |
Y2dcosts |
|||
|
Special social services |
Y3dcosts |
|||
|
Psychological support |
Y4dcosts |
|||
|
Independent factors, Хn |
||||
|
1 |
Long-term educational costs |
Х1 |
Secondary education (tutoring services) costs |
|
|
Vocational education (vocational school/college) costs |
||||
|
Higher education costs |
||||
Note – Compiled by the authors based on the results of mathematical modeling PLS3-PM
|
1 |
2 |
3 |
4 5 |
|
2 |
Additional government services |
Х2 |
Short-term “respite” services |
|
Long-term “respite” services |
|||
|
Other family services |
|||
|
3 |
Accessibility of healthcare and medicines for the child |
Х3 |
Volume of services |
|
Service quality |
|||
|
Terms of service (right to receive services, availability) |
|||
|
4 |
Accessibility of special social services for the child |
Х4 |
Volume of services |
|
Service quality |
|||
|
Terms of service (right to receive services, availability) |
|||
|
5 |
Other services according to the individual rehabilitation program |
Х4 |
Volume of services |
|
Service quality |
|||
|
Terms of service (right to receive services, availability) |
|||
|
6 |
Time spent by family members on child care, hours per day |
Х3 |
Mother |
|
Father |
|||
|
Other family members |
|||
|
7 |
Allowances |
Х7 |
One allowances |
|
To allowances |
|||
|
Three allowances or more |
|||
|
8 |
Family characteristics |
Х8 |
Per capita income |
|
Number of children in the family |
|||
|
Person who babysits the most |
ECONOMY Series. № 1(105)/2022
127
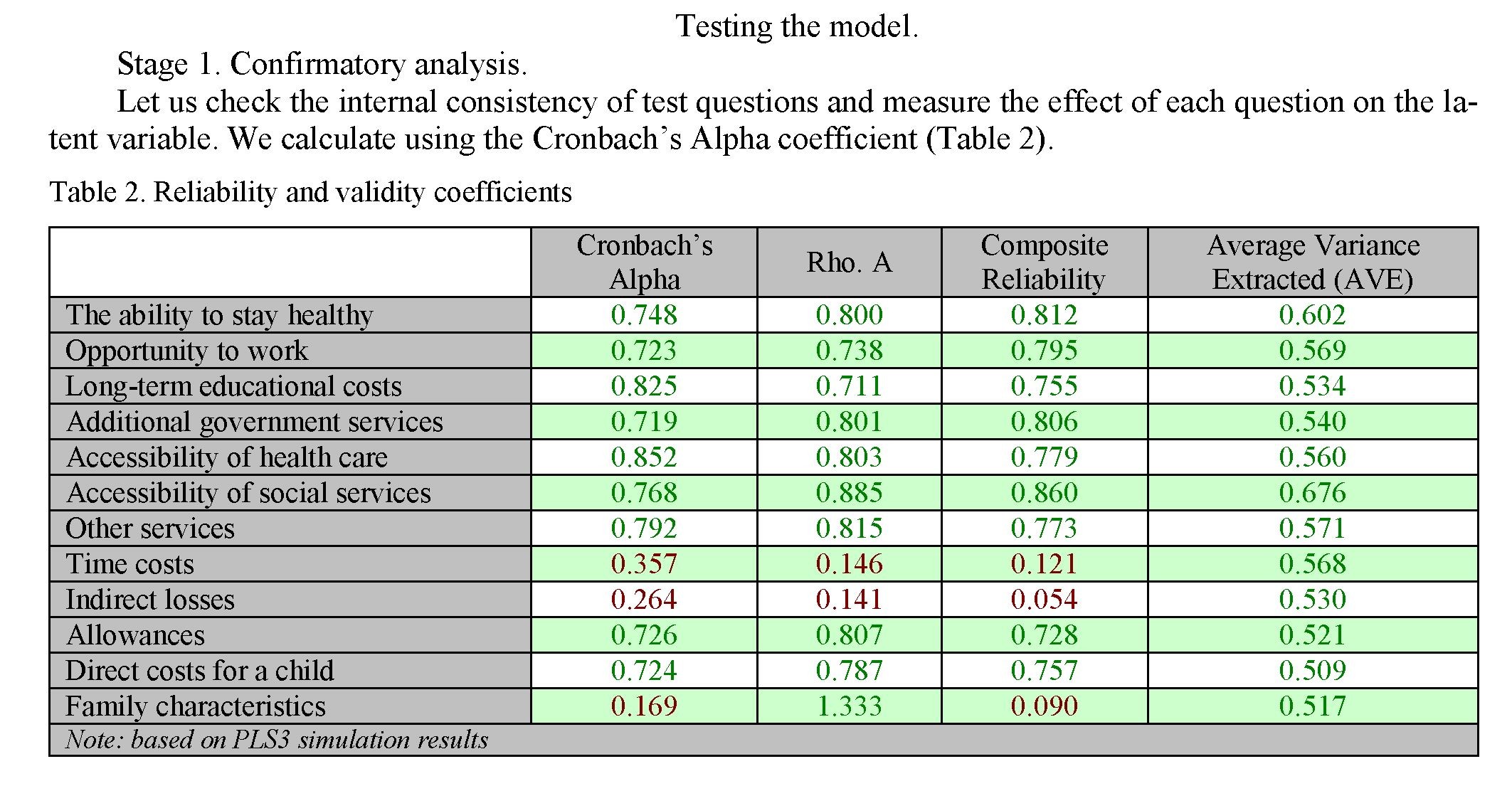
Cronbach’s Alpha serves as an indicator of the homogeneity (internal consistency) of indicator evaluation.
Coefficient scale is as follows:
- 0.5: low;
- 0.6: satisfactory;
- 0.7: good;
- 0.8: very good;
- 0.9: high.
- shows a fairly high level of internal consistency of the test elements and their impact on factors. The exceptions were “Time costs,” “Indirect family losses,” and “Family characteristics.” This is explained by the large spread of values and the heterogeneity of the responses received. In general, the Cronbach’s alpha shows high values, which indicates acceptable reliability statistics.
The Average Variance Extracted (AVE) is the variance of the indicator elements. The AVE value should be 0.5 or greater, but less than the Cumulative Reliability (CR). That is, the variance explained by the design should be greater than both the measurement error and cross-loads. Since AVE and the corresponding reliability coefficients are based on factor loads, their values vary depending on the factor model. The AVE for a factor or hidden variable should also be higher than its correlation square with any other factor or hidden variable.
Composite Reliability (CR) is the coefficient, which determines the overall reliability of the composition. It is calculated using the square of the sum of standardized factor loads and the sum of the error variance. The value of CR is in the range from 0 to 1, where 1 means absolute reliability. Threshold values of CR are as follows: 0.6 is suitable for exploratory studies, 0.7 is for confirmatory studies, and 0.8 or higher is good reliability for confirmatory studies. CR must exceed the AVE value.
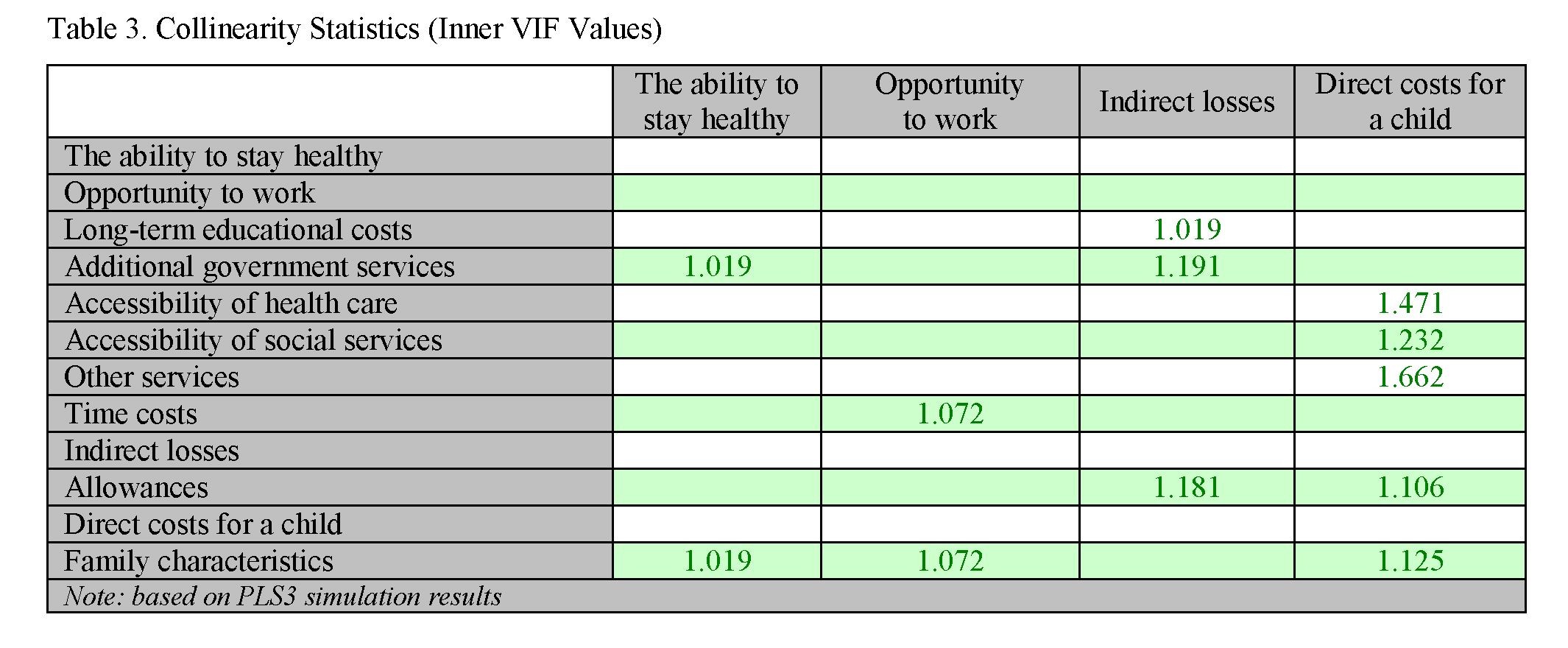
Collinearity check.
Collinearity means that there is a linear relationship between independent variables of the model. Factors that are closely related are withdrawn from the model, since they violate the condition of independence between explanatory variables. The remaining factor is the one that, with a sufficiently close connection with the result, has the least closeness of connection with other factors.
- shows the collinearity statistics obtained. To detect multicollinearity, the VIF indicator is used. Its maximum allowable value is 5, and the minimum threshold is 0.2.
128
Вестник Карагандинского университета

129
The data shown in Table 3 are in the acceptable range of values, which indicates variables are not multicollinear.
Determination coefficient.
Squared multiple correlation is the proportion of variance of a dependent variable explained by the model under study (by independent variables). The R-Squared has the range of 0 to 1. Dependence between dependent and independent variables increases with the coefficient’s approximation to one. In regression models, this means model matches to the data.
R Square Adjusted is the adjusted determination coefficient. It is used to compare models with a different number of factors in such a way that the number of factors does not affect the R-Squared statistics.
The correlation coefficient obtained in the model for the variable “The ability to maintain health” is 0.332. This means that about 33% of the variance of this model is explained by independent factors included in it (see Table 4).
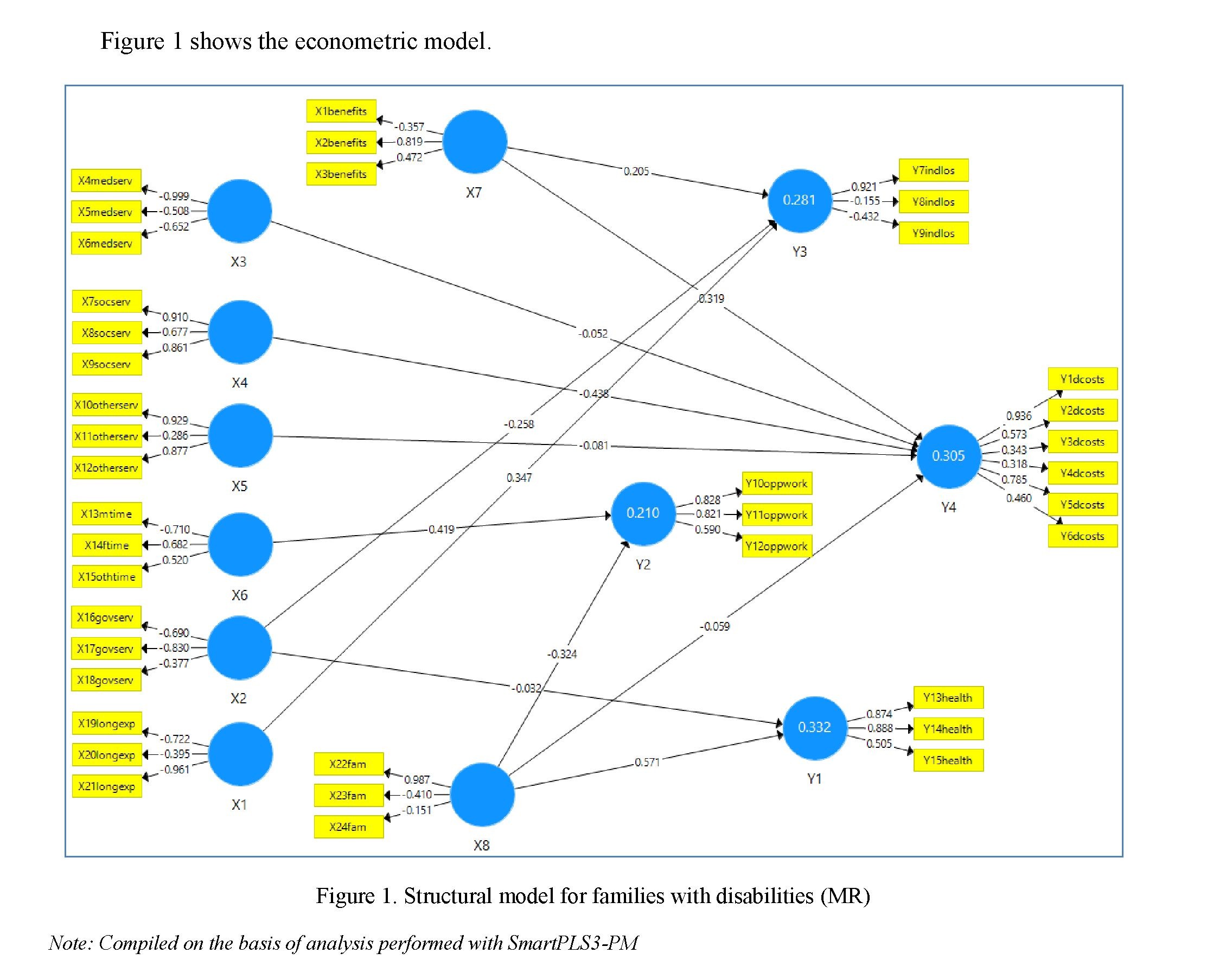
Let us consider the simulation results. As Figure 1 shows, the degree of interdependence of each of the impact factors has different values.
The Y1 variable (The ability to stay healthy) depends on the variables X2 (Additional government services: -0.032) and X8 (Family characteristics: 0.571.) According to the simulation results, the composition of the family has a significant impact on the parents’ ability to stay healthy. This is because the size of the average family income, the number of children in the family and the characteristics of the person who babysits the most have a direct and significant impact on the ability of family members (primarily those who care for the child) to stay healthy. Factor X2 has a weaker impact on Y1, because, according to the survey results, members of the family with a disabled child do not receive additional government free services, or receive an extremely small amount of them (additional leave for the second parent, community worker services twice a week for two hours, etc.). Thus, the influence on the ability to stay healthy in this case is weak.
The Y2 variable (Opportunity to work) depends on factors X8 (Family characteristics: -0.032) and X6 (Time spent on caring for a disabled child: 0.419). The time spent on caring for a child with developmental disabilities has a much greater impact on the family members’ opportunity to work. We can say that the factor of having a disabled child in the family negatively affects the working opportunities of parents or relatives. This becomes an important factor imposing restrictions on the family. As for X8, the degree of its impact on Y2 is lower, but is still significant. The family characteristics (income, the number of children, the disabled child caretaker) determine the parent’s working opportunities. For example, a grandmother often takes care of a disabled child, which allows her mother to start a job. Another common situation is when the child cannot be left for a long time without mother’s supervision, which limits her working opportunities completely. Ultimately, all of this also has a negative impact on the family’s welfare.
The Y3 variable (Indirect family losses). This variable directly depends on X7 (Allowances: 0.205), X2 (Additional government services: -0.258), and X1 (Long-term education costs: 0.347). According to the degree of impact, each of the factors has a different value. We can add X7 to the list of factors with minor impact. This is due to the fact that, according to respondents, at present, allowances have a significant impact on the well-being of the family and direct costs (more details below). Indirect losses are associated with the loss of income of one of the family members, or with the fact that additional costs are required for healthcare or counselling for parents. However, little money from the allowances received goes to these. Therefore, this factor’s impact on indirect family losses is insignificant. Also, additional government services for the family have a small impact on indirect losses. This is because the volume of such services is extremely small, and most often is non-existent.
X1 (Long-term education costs) has a significant impact (0.347) on indirect costs. This is due to the fact that the family allocates a fairly large amount of financial resources on education and development of the child even now, laying the groundwork. They often use the services of tutors, additional classes, paid secondary and higher education, etc. This imposes significant restrictions on ensuring the well-being of the family even now, because part of the income has to be redistributed to additional education services. When assessing long-term costs, parents associate them with indirect losses of the family.
The Y4 variable (Direct costs per child). This variable is of the greatest importance for the welfare of the family. As our survey showed, almost all families, with no exception, bear direct costs related to the health or education of a disabled child. Such costs have a direct impact on the family as a whole. The mathematical model showed that Y4 variable is influenced by factors X7 (Allowances: 0.319), X3 (Accessibility of health care: -0.052), X4 (Accessibility of social services: -0.438), X5 (Other services: -0.258), and X8 (Family characteristics: -0.059).
For families receiving allowances, they are extremely important for the well-being of the family as a whole. Many of the surveyed households receiving child disability allowances and care for a disabled child have noted that this source of income is their main one. Other sources are temporary and non-permanent. Therefore, allowances, their size and accessibility are one of the most important factors in ensuring the welfare of the family.
Availability of medical services (X3). This factor has little effect on the volume of direct costs. This is due to the fact that, in the total volume of direct costs, healthcare for children with MR takes only a small amount. If a family receives healthcare at its own expense, their share in expenses is significantly less than special social services (X4.)
Now, the value of special social services (X4) for direct costs is the greatest. This is the small amount of government services currently limited because of the accessibility of such services for the child. Therefore, family has to pay for such services from its own budget. Their cost is also high, i.e. their share in the total volume of direct costs is much greater than healthcare. The cost of such services may also be affected by the place of residence. For example, in rural areas, many special social services are unavailable due to their absence. Therefore, the family has to periodically travel to the city or receive home-based services, which also increases the final cost of such services. Thus, we can say that special social services, their accessibility and cost have an extremely strong impact on the family’s direct expenses and its welfare.
The value of X5 (Other services for the child) for direct costs is insignificant. This is because other services (for example, art therapy, hippotherapy, etc.) are most often not included in the rehabilitation package. Therefore, they do not affect the amount of direct costs.
The composition of the family also has a rather weak effect. The direct costs for a disabled child do not depend directly on babysitting person or the number of children in the family. However, in this case, the composition of the family and its completeness are indeed important. According to the results of our survey, almost three-quarters of families are complete. A quarter of them are incomplete and are basically just women. Here, the factor of income is the one imposing restrictions on improving the welfare of the family, because such families largely rely on allowances and/or on the mother’s side job. The completeness of the family and the opportunity of its members to work have a sufficiently significant impact on the well-being of the family as a whole.
131
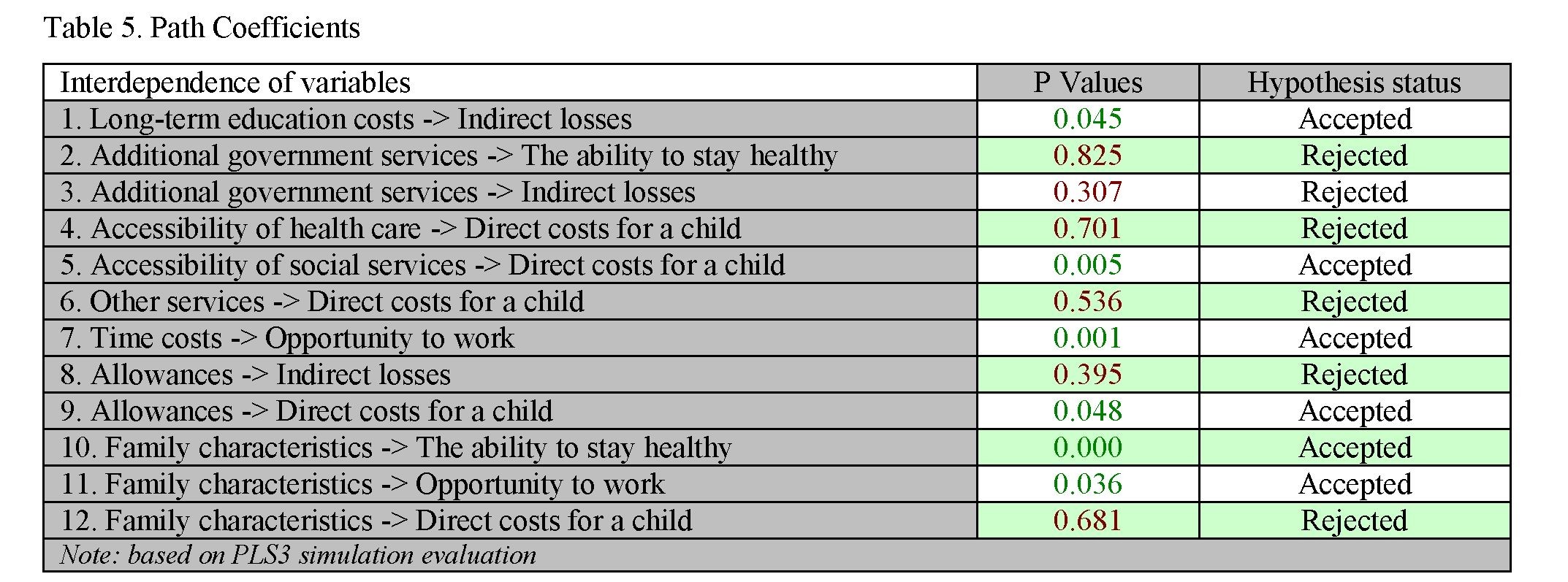
Stage 2. Hypothesis testing.
Thus, based on the results of constructing a mathematical model, we can determine the factors of the greatest or least impact on the well-being of the family with a disabled child, as well as the degree of their interdependence and impact on each other. Let us check the effectiveness of all the coefficients obtained. To do this, we use Bootstrapping, a command within SmartPLS, to test the statistical significance of the analysis results. The Bootstrapping procedure initiates verification and returns the result of the study gradually, from simple events to complex ones. This is how we find out the significance level of the coefficients and the reliability of the hypotheses set (Table 5).
Path Coefficients results have confirmed some of the presented interdependencies of family restriction factors and have not the other. In this vein, the “Long-term education costs -> Indirect losses” ratio has a clear statistical relationship. This suggests that the costs of educating a disabled child have a significant impact on indirect costs. For example, an increase in the cost of additional education may negatively affect the availability of other services for other family members.
The same is for the costs of additional social services. As the analysis showed, they have a clear connection with the direct costs for a child. Their size can have a significant impact on the well-being of the family, because sometimes the cost of such services is high, and their accessibility free of charge is limited.
We have also confirmed the hypothesis that the time spent on raising a disabled child and the opportunity to work have a direct relationship. The opportunity to work is also influenced by the composition of the family. So, if there is a possibility of shifting the responsibilities of raising a child to another family member, then the mother starts a full time or a part-time job. Also, this opportunity has a positive effect on the health support situation, the so-called possibility of a temporary respite.
Direct costs for a child with disabilities are affected by allowances, their number and size. The dependence is clear. Thuswise, we can say that allowances have the strongest impact on the welfare of a family with a disabled child. This conclusion is confirmed by the survey results. With no exception, all families who receive allowances note that this is an extremely important factor in ensuring the welfare of the household. For 24% of families, allowances are the main source of income.
According to the results of a number of studies, the main restriction factor for families with disabled children is an increasing financial burden. For instance, according to some researchers, a severe form of disability for a child increases the likelihood of spending 30% more on healthcare than if the child was born perfectly healthy. In certain countries, this burden is borne by the state, in particular, as compensation payments. Our study has shown that the increase in the financial burden on the family can be up to 25-30% of the average monthly income for a significant majority of households. In Kazakhstan, social benefits (allowances) are important just as well. Thus, we can say that the factor of an increasing financial burden on the family is one of the most important factors limiting its well-being both in Kazakhstan and in foreign countries.
Also, our research has confirmed the conclusions made by foreign scientists regarding the employment of at least one of the family members. Baydar, Joesch, et al. prove that about 15% of parents (one of the parents) have completely terminated their working activities due to the birth of a disabled child, and about 17.4% have switched their jobs to spend more time with the child. In Kazakhstan, the parental employment situation is just as difficult. So, before the birth of a child, 86% of surveyed women had jobs. After the birth of a child with developmental disabilities, 42% worked at the time of the survey, which is half as much. Thus, we can again argue that a decrease in the opportunity of parents of disabled children to work is a factor in reducing the welfare of both domestic and foreign families. Ultimately, these push families to reduce the size of disposable income and to poverty, as some foreign researchers point out (Porterfield, 2002; Kuhlthau & Perrin 2001; Powers 2001; Lukemeyer, Meyers & Smeeding, 2000.) The same situation is developing in Kazakhstan families. The opportunity to spend on healthcare and education decreases, the burden on the family budget increases due to the need to purchase additional services and medicines, the costly part of the budget is being restructured in favor of a disabled child and to the detriment of other family members’ interests, etc.
Every researcher claims that the birth of a child with a disability imposes restrictions on the development of both the family as a whole and each of its members separately. These restrictions have a fairly wide range: financial, economic, psycho-emotional, social, physical, etc.
Changes in the income level and the cost structure are an integral part of the life of a family with a disabled child. The birth of a child with disabilities has the greatest impact on the opportunity of family members to earn and on disposable income, as well as the structure of direct costs. In most cases, one of the parents terminates their work to care for a disabled child, or switches their job with a freer work schedule. It is important to note that the opportunity to work is significantly affected by the family characteristics, its completeness. If, for example, the family is incomplete, allowances become an important factor in ensuring the desired level of welfare for the family, where they are often the only source of permanent income. Thus, the direct costs for a disabled child can reach up to 25-30% of the total budget. The diagnosis of the child is of a great influence here as well. The results of mathematical modeling have shown that direct costs are the most important factors affecting the well-being of a family with disabilities. We have confirmed the hypothesis on the impact of allowances on direct costs.
One of the important factors restricting the development of a family with disabled children are indirect losses associated with a reduction in income from employment of a family member who babysits the most, the need to buy additional paid healthcare/counselling and other services for the parent. However, unlike direct losses, allowances have less impact on indirect losses. This is due to the fact that indirect losses of a family from the birth and raising a disabled child may “manifest” after a while, while allowances and their size have a direct impact on current costs. Much more important here are the additional costs of addressing the future issues (healthcare, education, etc.). Parents understand these services are required now, so they are ready to spend part of the family budget on them now. They hope such costs will have a positive effect on the quality of life of a child with disabilities in the future.
An important factor in the well-being of a family is the ability of its members to stay healthy. This is especially true for those family members who take care of a disabled child. As mathematical modeling shows, the factor “family composition (complete or incomplete)” is of the greatest importance here. A full family has more opportunities to free one of the family members from the responsibilities of caring for a disabled child, at least for a while. This allows using the freed time to stay healthy. For single-parent families, this opportunity is sharply reduced, and the unavailability of temporary respite services for the parent is of a great importance.
As mentioned above, sometimes the birth of a disabled child negatively affects the parents’ opportunity to work. The time spent on caring for a disabled child has a significant impact here. The more severe the diagnosis, the less independence such a child has, the less likely it is that the parent will start a job. This will again have a negative impact on the well-being of the family as a whole. Therefore, the factor of completeness of the family is of great importance when there is a possibility to shift part of caring responsibilities to other family members (e.g., a grandmother).
We plan to develop mechanisms to neutralize or prevent the identified restrictions in the nearest future.
Acknowledgements
The results of the study have been obtained within the framework of the grant funded project supported by the Committee of Science of the Ministry of Education and Science of the Republic of Kazakhstan “The system of support for households with disabled children: Conceptual foundations, effective practices, development mechanisms in Kazakhstan,” 2020-2022. Registration no. AP0880566.
References
- Sait Agenstva po strategicheskomu planirovaniu i reformam Respubliki Kazakhstan [Site of Agency for Strategic planning and reforms of the Republic of Kazakhstan]. bala.stat.gov.kz. Retrieved from
- https://bala.stat.gov.kz/chislennost-detej-invalidov-ot-0-do-17-let-vklyuchitelno/ [in Russian].
- Bajserkina, F. (2013). Fizicheskaia reabilitatsiia zdorovia detei-invalidov na sovremennom etape [Physical rehabilitation of the health of disabled children at the present stage]. Astaninskii meditsinskii zhurnal — Astana Medical Journal, 4, 93–97 [in Russian].
- Carissa, A., Gottlieb, MS., Matthew, J., Maenner, BS., Claudia, Cappa MPhil., Prof Maureen & S. Durkin PhD (2009). Child disability screening, nutrition, and early learning in 18 countries with low and middle incomes: data from the third round of UNICEF’s Multiple Indicator Cluster Survey (2005-06). The Lancet, 374, 1831–1839.
- Ejdemiller, E.G. (2008). Psikhologiia i psikhoterapiia semi [Family psychology and psychotherapy]. Saint Petersburg [in Russian].
- Elfimova, N.V. (1978). Sravnitelnoe izuchenie uslovii obrazovaniia obobshcheniia u doshkolnikov s normalnym i zaderzhannym razvitiem [Comparative study of the conditions for the formation of generalization in preschoolers with normal and delayed development]. Candidate’s thesis. Moscow [in Russian].
- Emelina, D.A., & Makarov, I.V. (2018). Zaderzhki psikhicheskogo razvitiia u detei (analiticheskii obzor) [Delays in mental development in children (analytical review)]. Obozrenie psihiatrii i medicinskoi psikhologii — Review of Psychiatry and Medical Psychology, 1, 4–12 [in Russian].
- Sait «Federalnyi reestr invalidov Rossii» [Site Federal Register of Disabled Persons of Russia]. sfri.ru. Retrieved from https://sfri.ru/analitika/chislennost/chislennost-detei?territory=undefined [in Russian].
- Forsakringskassan. (2021). Swedish insurance system. Retrieved from https://www.forsakringskassan.se
- Giulio, P., Philipov, D., & Jaschinski, I. (2014). Families with disabled children in different European countries. Families and Societies. Working Paper Series.
- Goloshchapov, A.V. (2016). Zarubezhnye metody profilaktiki i korrektsii zaderzhek psikhicheskogo razvitiia u detei. Metod ritmicheskoi stimuliatsii H. Blomberga i neirofiziologicheskoi integratsii neonatalnykh refleksov S.G. Blait [Foreign methods of prevention and correction of mental retardation in children. Method of rhythmic stimulation H. Blomberg and neurophysiological integration of neonatal reflexes S.G. Blythe]. IX Mezhdunarodnaia nauchno- prakticheskaia konferentsiia Psihologicheskoe soprovoghdenie obrazovania: teoria i practika, (01-02 aprelia 2020) — IX International Scientific and Practical Conference. (pp. 103-108). Yoshkar-Ola [in Russian].
- Kirton, D. (2009). Child social work policy & practice. London: SAGE Publications Ltd. 240.
- Kobernik, G.I., & Sinev, V.N. (1984). Vvedenie v spetsialnost defektologiia [Introduction to the specialty defectology]. Kiev [in Russian].
- Kovalev, V.V. (1979). Psikhiatriia detskogo vozrasta (rukovodstvo dlia vrachei) [Child psychiatry (guide for doctors)]. Moscow: Meditsina [in Russian].
- Langerman, C., & Worrall, E. (2005). Ordinary lives: disabled children and their families: a guide for donors and funders. New Philanthropy Capital.
- Lea Anne. DeRigne, Shirley. L., & Porterfield, P. (2015). Employment Change Among Married Parents of Children With Special Health Care Needs. Journal of Family, 1, 28.
- Lebedinskaya, K.S. (2006). Osnovnye voprosy kliniki i sistematiki zaderzhki psihicheskogo razvitiia [The main issues of the clinic and systematics of mental retardation]. Defektologiia — Defectology, 3, 15–27 [in Russian].
- Lukemeyer, An., Meyers, M., & Smeeding, T. (2000). Expensive Children in Poor Families: Out-of-Pocket Expenditures for the Care of Disabled and Chronically Children in Welfare Families. Journal of Marriage and Family, 62(2), 399–415. Doi: 10.1111/j.1741-3737.2000.00399.x.
- Mezhdunarodnyj opyt organizatsii sistemy sotsialnoi pomoshchi. Na primere piati stran [International experience in organizing the social assistance system. Using the example of five countries]. (2004). Moscow [in Russian].
- Morris, Z., & Zaidi. A. (2020). Estimating the extra costs of disability in European countries: Implications for poverty measurement and disability-related decommodification. Journal of European Social Policy, 30(3), 339–354.
- Doi: 10.1177/09589287198 91317.
- Muzaparova, L.M. (2003). Polozhenie invalidov v Kazakhstane: problemy i puti sotsialnoi reabilitatsii [Situation of disabled people in Kazakhstan: problems and ways of social rehabilitation]. Analytic, 5, 29–30 [in Russian].
- National Institute of Statistics, Geography and Information of Mexico. (2021). Рeople with disabilities 2014. Retrieved from https://www.inegi.org.mx/app/biblioteca/ficha.html?upc=702825090203
- Office for National statistics. (2021). Analysis exploring the lives of disabled people in the UK, to understand disparities and investigate causalities. Retrieved from https://www.ons.gov.uk/peoplepopulationandcommunity
- /healthandsocialcare/disability.
- Okon, M., Henderson, A., Kinnear, D., & Cooper, Sally-Ann. (2019). Trends and variations in per capita expenditure on adult intellectual disabilities health and social care across Scotland, and by urban/rural class. Journal of Applied Research in Intellectual Disabilities, 32(1), 121–130. Doi: 10.1111/jar.12514.
- Parish, S.L., Shattuck, P.T., & Rose, R.A. (2009). Financial burden of raising children with special health care needs: Association with state policy choices. Pediatrics, 124, 435–442.
- Pevzner, M.S. (1972). Klinicheskaia kharakteristika detei s zaderzhkoi razvitiia [Clinical characteristics of children with developmental delay]. Defektologiia — Defectology, 3, 3–9 [in Russian].
- Tkacheva, V.V. (2014). Semia rebenka s ogranichennymi vozmozhnostiami zdorovia: diagnostika i konsultirovanie. [The family of a child with disabilities: diagnosis and counseling]. Moscow [in Russian].
- UNICEF. (2013). Children with Disabilities. Retrieved from https://www.unicef.org/media/84886/file/SOWC- 2013.pdf.
- Statistical data bank of Moldova. (2021). Persons with disabilities. Retrieved from https://statbank.statistica.md/PxWeb/pxweb/en/30%20Statistica%20sociala/
- Statistisches Bundesamt. (2021). Database of the Federal Statistical Office of Germany. Retrieved from https://www- genesis.destatis.de/genesis/online?operation=abruftabelleBearbeiten&levelindex=1&levelid=1633417891741& auswahloperation=abruftabelleAuspraegungAuswaehlen&auswahlverzeichnis=ordnungsstruktur&auswahlziel=wert eabruf&code=22711-0002&auswahltext=&werteabruf=Werteabruf#abreadcrumb [in German].
- Sergeeva, O.A., Filippova, N.V., & Barylnik, Yu.B. (2015). Problema psikhologicheskoi gotovnosti k shkolnomu obucheniiu detei s zaderzhkoi psikhicheskogo razvitiia [The problem of psychological readiness for schooling children with mental retardation]. Bulleten medicinskikh internet-konferentsii — Bulletin of medical Internet conferences, 5, 712 [in Russian].
- Stabile, M., & Allin, S. (2012). The economic costs of childhood disability. Future Child. Princeton University, 22(1). 65–96.
- Vlasova T.A., & Lebedinskaya, K.S. (1975) Aktualnye problemy klinicheskogo izucheniia ZPR u detei [Actual problems of clinical study of IMF in children]. Defektologiia — Defectology, 6, 8–17 [in Russian].
- World Health Organization. (2011). World Bank. World report on disability. Retrieved from http://www.who.int/disabilities/world_report/2011/en/index.html
- World Health Organization. (2020). Disability and health. Retrieved from https://www.who.int/ru/news-room/fact- sheets/detail/disability-and-health
- Zaidi, A., & Burchardt, T. (2005). Comparing incomes when needs differ: equivalization for the extra costs of disability in the U.K. Rev Income Wealth, 51, 89–114.