In this article, we will introduce and discuss new options by using personal decision support and e-health services in diabetes management. Usage of the KADIS® system for personal decision support provides opportunities to identify improved therapy options in accordance with the guidelines of the professional societies. This enables the best treatment modality for the individual patient to be determined in a very short time and, individual circumstances of the patient as well as the practical feasibility of treatment recommendations are taken into account. Furthermore, the telemedicine platform TeleDIAB® together with the embedded KADIS® simulation are suitable to make knowledge and experience globally available to treat diabetes.
Introduction
According to data, recently published by the International Diabetes Federation (IDF), an estimated 371 million persons worldwide have diabetes mellitus. Four out of 5 diabetes patients live in developing and emerging countries. Especially in Asia and in countries of the Gulf region with a high population growth rate and drastical changes in living conditions, the disease has reached an epidemic dimension. The diabetes prevalence in these regions already exceeds 20 % [1–3]. Prevalence figures also rise, even though not to the same extent, in developed countries, like the U.S. and Germany; however, other factors, such as an aging society, overnutrition, and lack of physical activity may play a role. In contrast to developing and emerging countries, significantly larger healthcare budgets are available in highly-developed countries for diabetes treatment. Furthermore, within the latter healthcare systems extensive know-how and sophisticated treatment strategies have been established for management of diabetes. This includes research, established structures of diabetes care, and special programs aiming to prevent diabetes.
Thus, general practitioners as well as diabetes specialists can take advantage of a wide variety of pharmaceutical and technical resources available for diabetes treatment. Guidelines have been established by the ADA and EASD in order to standardize diabetes care [1, 4]. With data provided by blood glucose selfmonitoring, continuous glucose monitoring systems or collection of self-control data by the patient, and numerous diagnostic parameters needed for treatment decisions, the doctor is faced with a huge amount of information. For the evaluation of glucose variability, for example, alone over 30 different metrics have been published until now [5–11].
The increasing prevaalence of diabetes, the great variety of treatment options, and the flood of data raise the necessity of appropriate and effective strategies applicable to find a timely therapeutic approach tailored to the individual needs of the patient. As our previous outcomes showed, the telemedicine-based Karlsburg DIiabetes management System KADIS® could play an important role [5, 6] in achieving this goal. In addition, telemedicine solutions are suitable to make knowledge and experience globally available to treat diabetes.
Karlsburg Diabetes Management System, KADIS®
The metabolic status is as different as a fingerprint for each person and clearly shows an individual rhythm reflected in the 24-h blood glucose curve of a patient. By means of KADIS®, a so called in silico copy of the metabolic behavior of diabetic patients can be created for the first time worldwide. The KADIS® system itself is protected by patents, but its application was already published in peer-reviewed journals [12, 13].
To map the individual metabolic behavior in silico, i.e. in a computerbased model, the KADIS® system requires data, which can be easily collected under everyday conditions. This includes blood glucose readings, patient’s self-control data, such as glycemic therapy (insulin, oral antidiabetics), food intake as well as physical activities (sports) and demographic data (e.g., age, diabetes type, disease duration, body weight and height). After entering all these data, they will be automatically analyzed by the KADIS® system. Upon information on dose and insulin formulations or oral drugs, the corresponding activity profiles are calculated, absorption profiles for food intake be determined, and sports activities are converted into insulin action equivalents. Importantly, the insulin responsiveness during the day can be visualized. Moreover, in the case of Type 2 diabetes, the daily profile of endogenous insulin can be determined and simultaneously displayed with the insulin responsiveness by means of the KADIS® model. During the subsequent iteration process, blood glucose curves will be simulated on the basis of the available data. The specific parameters of the KADIS® model are gradually adapted based on a patented mathematical method until defined termination conditions are reached. As a result of this procedure, one obtains a setting of the KADIS® system, where the blood glucose tracings of the patient derived from glucose monitorings is best reflected by the simulated glucose profile. The in silico mapping of the individual metabolic behavior on the PC is referred to as personal «Metabolic fingerprint» of the patient (Fig. 1).
Blood glucose tracing obtained from 24-hour glucose monitoring (red dotted line); 24-hour insulin activity profiles (total insulin available) exogenous insulin (blue area) and endogenous insulin (light blue area); insulin sensitivity throughout the day (pink curve); 24-hour resorption profile of meals (light brown area), insulin and oral drugs intake (time, dose, type); meals (food, quantity, time)
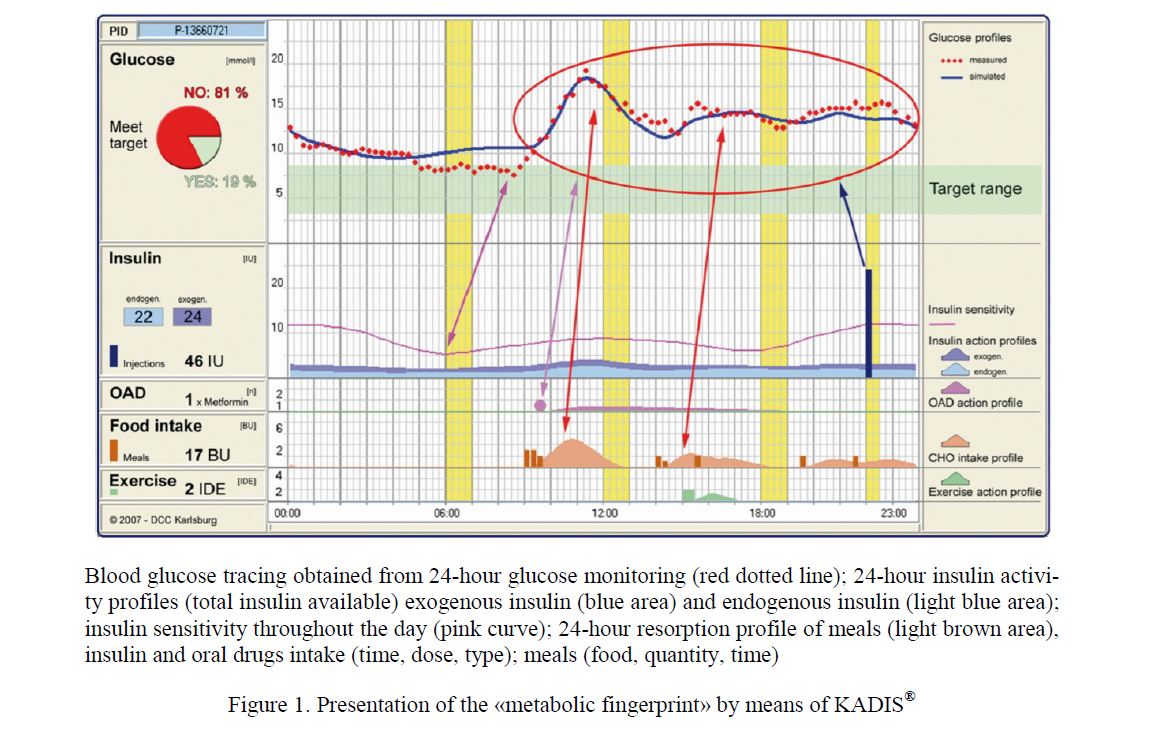
Figure 1. Presentation of the «metabolic fingerprint» by means of KADIS®
Weak-point Analysis
Weak points, such as hypoor hyperglycemia can be read directly in the course of blood glucose changes from the «metabolic fingerprint» (Fig. 1). Using KADIS®; however, a more sophisticated analysis of potential weak points can be performed. A causal relationship of hyperglycemia/hypoglycemia with current therapy (action profiles, time regime), with food intake (carbohydrate units), with physical activity and special events can be established. For example, rising blood glucose levels in the morning, before the first meal, could be explained by a significantly reduced insulin sensitivity and/or insufficient administration of exogenous insulin. Such a specific analysis of weak points induced by such factors is another unique feature of KADIS®.
Decision support, testing therapy recommendations
Based on the in silico mapping and weak point analysis, modelbased simulations of the blood glucose curve could be performed in terms of a decision support. Therapy changes envisaged by the diabetes care giver will be entered into the KADIS® system, which then simulates immediately the corresponding glucose curves for the entered data. Thus, the usual time-consuming and tedious «trail and error» approach can be circumvented. Strategies and therapeutic options recommended by guidelines of professional societies [1] can quickly and safely be tested in an interactive dialogue with the KADIS® system. This enables the best treatment modality for the individual patient to be determined in a very short time and, individual circumstances of the patient as well as the practical feasibility of treatment recommendations are taken into account. The results of this testing and individual treatment options are automatically documented in the KADIS® Report. This report is available either online or as download for use by the attending physician to adjust the patient´s glycemic therapy (Fig. 2).
The test shown in the figure demonstrates significant improvement of the blood glucose curve and the glycemic control to be expected (blue curve vs the original gray and red represented blood sugar curve). The percentage of time, where the patient is hyperglycemic, drops down from 100 % to 18 % (see «quality eye» in the upper right corner).
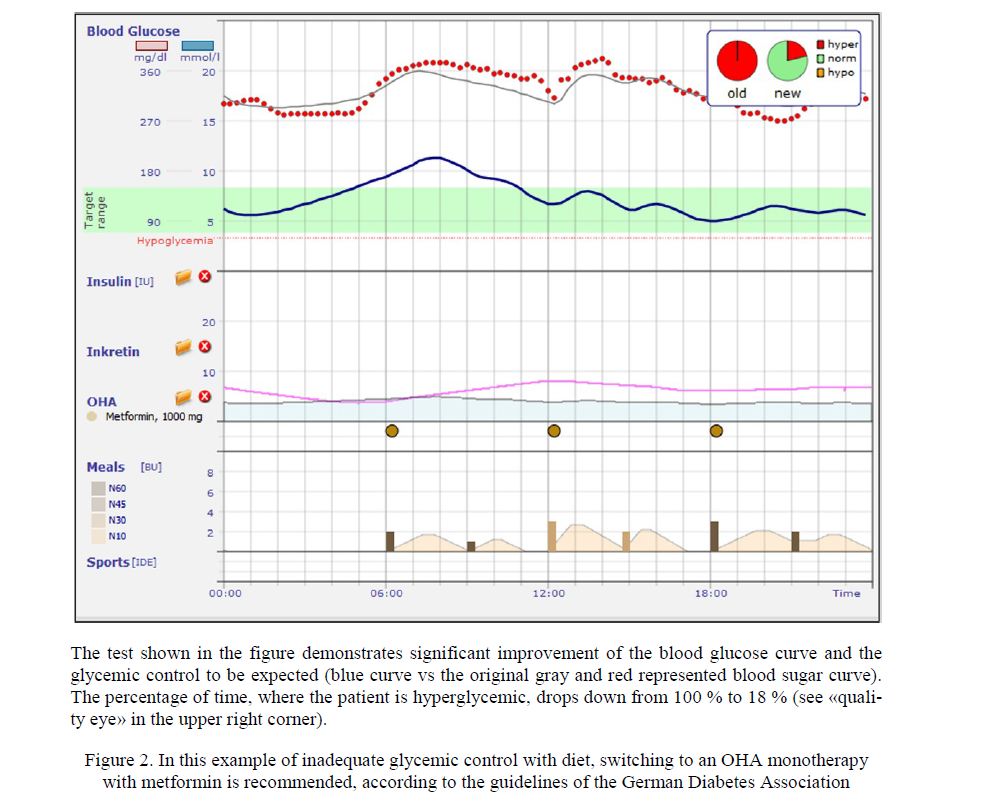
Figure 2. In this example of inadequate glycemic control with diet, switching to an OHA monotherapy with metformin is recommended, according to the guidelines of the German Diabetes Association
TeleDIAB® — E-Health Platform
To give GP’s as well as Diabetologists full access to the KADIS® functionality described above, the e-health platform «TeleDIAB®» was developed. TeleDIAB® is based on a high-performance secured database and is provided as a browser-based solution via the Internet. The Diabetes Service Center Karlsburg, as operator of the e-health platform, provides appropriate access accounts on the basis of licenses. In addition to the KADIS® simulation, the required routines for the acquisition of basic and self-control data are integrated in the TeleDIAB® platform (Fig. 3).
As soon as all necessary data has been collected, the KADIS® simulation component is ready to simulate glucose profiles. Depending on the design of the access to the TeleDIAB® platform, recommendations of diabetes experts can be provided and added to the start settings of the KADIS® system (KADIS® Identification). Up to 7 variants of tested therapy options can be stored simultaneously in TeleDIAB®. A brief note may be entered, explaining each simulation in order to allow better identification (Fig. 4).
The schedule representing the basic data is shown on the left, the right contains the Graphical User Interface (GUI) for recording blood glucose readings from glucose meter measurements and the corresponding self-control data, including therapy modalities and meals. In the case that CGM systems are used for recording of blood glucose, the glucose data will be uploaded to the TeleDIAB® platform.
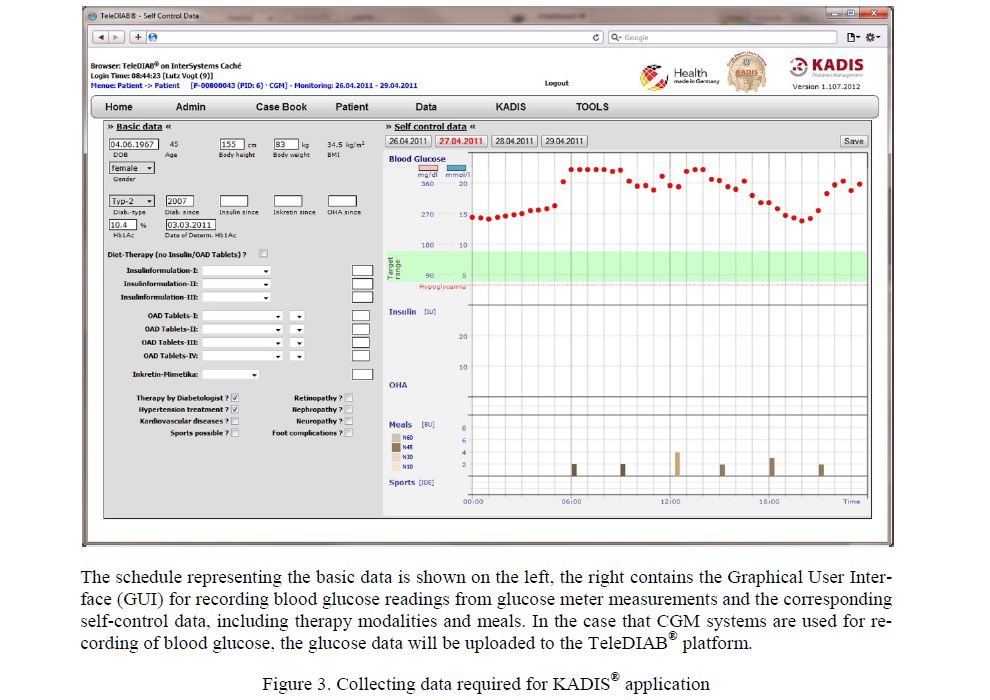
Figure 3. Collecting data required for KADIS® application
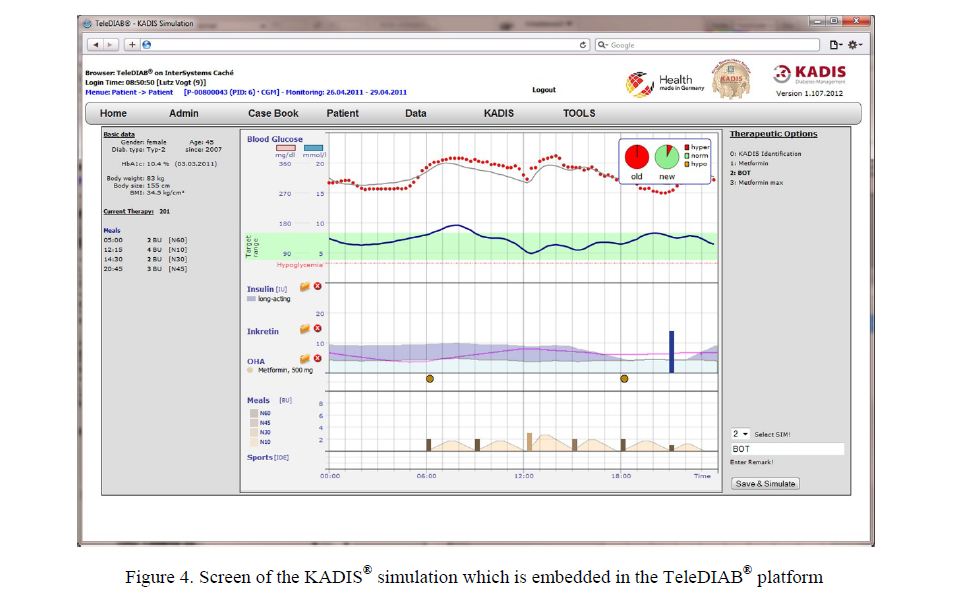
Figure 4. Screen of the KADIS® simulation which is embedded in the TeleDIAB® platform
The KADIS® Report summarizes the analysis of blood glucose monitoring, outcome of the KADIS® identification, and results of the simulation for recommendations of treatment options. The report is created automatically and can be read either online or downloaded as a PDF file (Fig. 5).
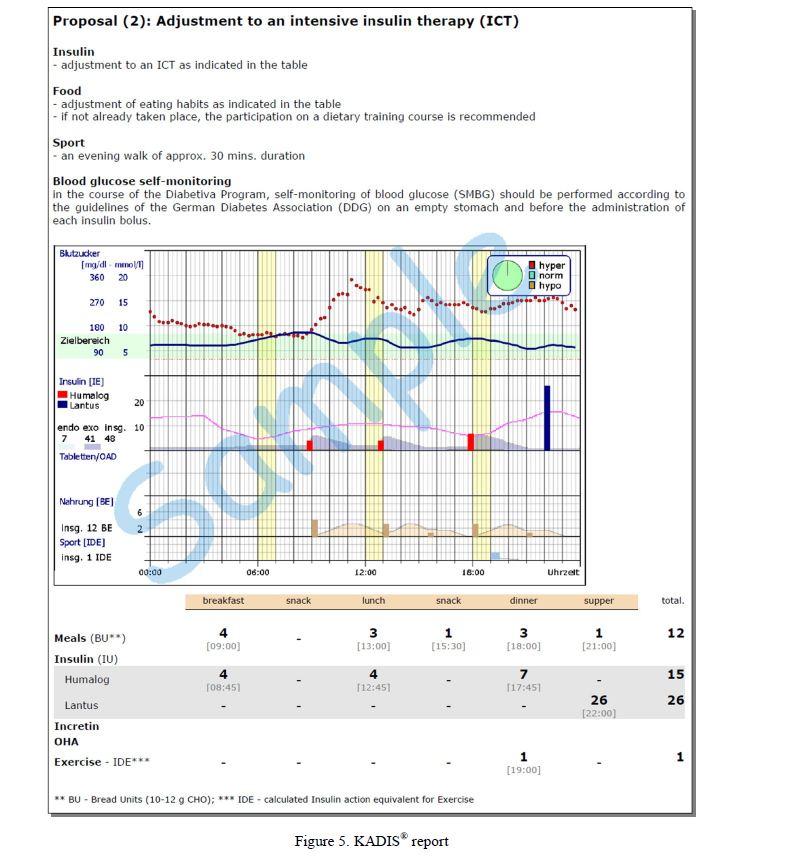
Figure 5. KADIS® report
Benefit analysis
The value benefit analysis will be released, provided that, as in the past, only the attending physician is to decide the treatment modalities. The main differences to generally accepted treatment practice are:
- Predictability of the therapy efficacy (e.g., avoidance of hypoglycemia, percentage of blood glucose values in target range) is achieved with KADIS® online immediately (within seconds), without loosing time until the next patient´s physician consultation for evaluating therapy outcome. This significant time saving helps, especially those patients with complicated diabetes.
- As patients can be involved via KADIS® Online in the process of optimization, the clear and visible identification of weak points in glycemic control on the KADIS® report, stimulates the interest in taking an active part in the improvement of metabolic control and makes the therapeutic approach better understandable.
- By bringing all important data for glycemic control on a single print sheet together, the doctor in attendance is able, at a glance, to assess individual metabolic characteristics of the patient and the efficacy of the therapeutic approach in
- The doctor can also consider alternative therapeutic approaches and is thus supported in its competence to find out the optimal treatment for his
Finally, the benefit through improved metabolic control in gaining personal quality of life and reducing the risk of late diabetes complications, as has been shown by the large diabetes studies DCCT and UKPDS, cannot be overemphasized.
Conclusions
Diabetes mellitus is a global problem of epidemic dimension. The determinants of the increasing prevalence of diabetes are different in each country. For several reasons, there are also considerable differences in the level of diabetes care. Telemedicine is a tool to make knowledge and experience in the treatment of diabetes globally available. The use of the KADIS® system, the world's unique computer program for diabetes management, enables care givers to examine personalized treatment recommendations and quickly and safely to find out the best treatment strategy for optimizing a patient`s glycemic control. With the embedding of KADIS® functionality in the telemedicine information system TeleDIAB®, essential conditions are met for using KADIS®, particularly in regions of the world where there is a need for evidence-based personalized medicine.
References
- Inzucchi E., Bergenstal R.M., Buse J.B., Diamant M., Ferrannini E., Nauck M., Peters A.L., Tsapas A., Wender R., Matthews D.R.; American Diabetes Association (ADA); European Association for the Study of Diabetes (EASD). Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) // Diabetes Care. — 2012. — Vol. 35, No. 6. — P. 1364–1379.
- Guariguata L., Whiting D., Weil C., Unwin N. The International Diabetes Federation diabetes atlas methodology for estimating global and national prevalence of diabetes in adults // Diabetes Res. Clin. Pract. — 2011. — Vol. 94, No. 3. — P. 322–332.
- Whiting D.R., Guariguata L., Weil C., Shaw J. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030 // Diabetes Res. Clin. Pract. — 2011. — Vol. 94, No. 3. — P. 311–321.
- Harris P., Mann L., Phillips P., Webster C. Diabetes management in General Practice. IDF 2012/13.
- Salzsieder , Vogt L., Kohnert K.D., Heinke P., Augstein P. Modelbased Decision support in Diabetes Care // Comput. Methods Programs Biomed. — 2011. — Vol. 102, No. 2. — P. 206–218.
- Augstein , Vogt L., Kohnert K.D., Heinke P., Heuzeroth V., Salzsieder E. The Karlsburg Diabetes Management System: from discovery to application // Res. Adv. In Diabetes Care. — 2009. — No. 1.
- Kohnert D., Heinke P. et al. Reduced glucose variability is associated with improved quality of glycemic control in patients with type 2 diabetes: a 12-month observational study // J. Endocrinol. Metab. — 2011. — Vol. 2, No. 1. — P. 64–72.
- Kohnert K.D., Vogt L., Salzsieder E. Advances in understanding glucose variability and the role of continuous glucose monitoring // European Endocrinol. — 2010. — Vol. 1, No. 6. — P. 53–56.
- Rodbard D. Interpretation of continuous glucose monitoring data: glycemic variability and quality of glycemic control // Diabetes Technol. Ther. — 2009. — Vol. 11, Suppl. 1. — P. S55–S65.
- Cameron F.J., Donath S.M., Baghurst P.A. Measuring glycemic variation // Current Diabetes Rev. — 2010. — Vol. 1, No. — P. 17–26.
- Fritzsche , Kohnert K.D. et al. The use of a computer program to calculate the mean amplitude of glycemic excursions // Diabetes Technol. Ther. — 2011. — Vol. 3, No. 13. — P. 319–325.
- Augstein P., Vogt L., Kohnert K.D., Freyse E.J., Heinke P., Salzsieder E. Outpatient assessment of Karlsburg Diabetes Management System-based decision support // Diabetes Care. — 2007. — Vol. 30, No. 7. — P. 1704–1708.
- Augstein P., Vogt L., Kohnert K.D., Heinke P., Salzsieder E. Translation of personalized decision support into routine diabetes care // J. Diabetes Sci. Technol. — 2010. — Vol. 4, No. 6. — P. 1532–1539.