A national or universal health care — the concept is rather vague, and in practice it is implemented in different ways. The health care system in each country — a product of its unique characteristics, history, political process, and the national character of the people, and many of these systems are currently undergoing major reforms. Analysis of the health system in Kazakhstan showed that, at present, to improve the quality of care recognized as a priority task, and Kazakhstan has already taken steps in this direction by promoting the principles of evidence-based medicine, developing and implementing new clinical guidelines, and implementing quality improvement processes at the level of health care provider. Preliminary results of the State Reform and Development Program of Health of the Republic of Kazakhstan for 2005–2010 indicate that progress in improving the quality of care, but further efforts are needed in this direction. Kazakh Government also recognizes the need to strengthen health promotion and disease prevention.
In the conditions of transformation of the Kazakhstan economy to the market there is a number of the problems concerning level of living of the population. The health care system is the integral indicator reflecting level of living of the population, promoting improvement of quality of life and society development as a whole. Providing the main medical authorities is a paramount form of investment in a human capital and an important factor of economic growth of the country.
A main goal of health protection is maintenance of long active life which is reached by preserving and strengthening of physical and mental health of each person, provision to it medical care in case of health loss. The inherent right to health protection, is provided with protection of high quality of food, and also provision to the population of the available medico-public assistance.
A priority there shall be a forming of system of health protection, and all its components shall become independent subsystems. The system of health protection shall be determined by the indicators characterizing each its component. In this case there will be a real possibility to estimate influence on health of the population of all components included in system, including health cares. Now are least developed financially the economic indicators, allowing to estimate influence on health of factors of social and economic wellbeing, a healthy lifestyle, ecology
In a basis of forming of systems of health protection and health care principles of the state responsibility for health of citizens and responsibility of citizens for the health shall be pledged. Upgrade and increase of efficiency of health care proceeding from the main priority — preserving and strengthening of health of the person is necessary. The being created market relations on the basis of different types of a property changed health care as social institute in which there were former principles of financing of a network of organizations in case of decrease in relative indicators of their security by financial resources. Thus public institutions of health care are forced to purchase material resources at market prices. There was an imbalance of the income and expenses of organizations. So far health care development in our country didn't purchase nature of dependence on needs of citizens, as consumers of medical care. The person didn't become the central figure when forming legal relationship on receipt of medical care. Needs of the person, the states directed on providing necessary level of health, didn't become a basis of forming of organizational and economic model of health care [1].
As show researches, despite measures undertaken by the state, conceptual mistakes and distortions in health care development meet. Ministry of Health of the Republic of Kazakhstan still has no accurate vision of final model of the Kazakhstan health care. In this regard, in September, 2009 the Code of the Republic of Kazakhstan «About health of the people and a health care system», directed on legislation ordering in the field of health care, its harmonization with the international norms and standards, increase of the status of national medicine, quality of rendering of medical care and level of medical attendance of citizens is accepted.
In our opinion for situation correction, at an initial stage follows: to provide population participation as a health care market regulator through real implementation of an option of the medical organization and the doctor; to implement the wages system of the medical workers based on economically counted quality standards of treatment; to pass from a principle of content of medical institutions to a principle of payment of specific amounts of rendering of medical care; to modernize system of primary medicosanitary help by construction new and reconstruction of existing objects of PMSP with wide integration into them specialized and social services; to move a part of amounts of rendering of medical care from a stationary stage on out- patient, to reduce a part of excessive capacities of hospitals, to enter a stage of rehabilitation treatment; to provide support to private medicine and others [2].
The analysis of foreign sources show that in the world practically there is no country where one of the listed sources of financing of health care would be used only. Everywhere there are mixed systems where this or that source of collection of the income prevails. Specialists consider that the source of financing shall correspond to activities of health care and functions carried out by these industry, thus the state shall bear responsibility for provision practically all services of public health care and certain types of clinical servicing (Table 1).
The Main activities of a health care system and sources of their financing
T a b l e 1
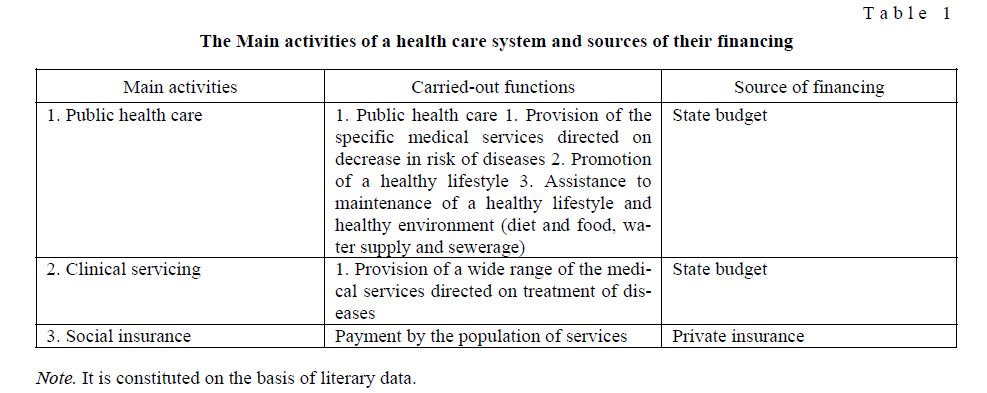
Note. It is constituted on the basis of literary data.
In this regard, in order to build an optimal organizational structure and financial model for health care, guaranteed availability and the quality of medical care, and three levels of funding: the first level is a guaran- teed amount of free medical care, funded from the state budget; The second level, a mandatory medical in- surance; the third level — the voluntary medical insurance services that are not provided for in the sugar free medical assistance, and program of compulsory health insurance, as well as pay-per-view services. The main load health financing in Kazakhstan are the budgets of all levels, with faster growing costs in the government budget. This is because, first of all, with the expansion of the programs providing costly high-tech types of medical assistance, targeted programs, as well as to the direction of funds on the financing of medical sci- ence, education, and the individual categories of citizens on the level indicators, reflecting the health of the population, have an impact the following external and internal factors.
External factors: According to WHO health rights on the 50 % depends on the lifestyle (socio-economic factors, level of education, the commitment to harmful habits, healthy lifestyles and other); up to 20 per cent of health depends on the state of the environment. Currently, only 81.8 % of the population provided safe drinking water, which in turn is reflected in the high-level infectious morbidity.
In Kazakhstan for the seven leading risk factors accounted for almost 60 % of the overall burden of in- fectious and chronic diseases: tobacco smoking (13.4 %), alcohol consumption in dangerous doses (12.8 %), high blood pressure (12.3 %), patients with congenital hypercholesterolemia (9.6 %), excessive weight (7.4 %), insufficient consumption of fruit and vegetables (5.5 %), low physical activity (3.5 %).
Currently, a low level of public health is the lack of awareness and motivation of the population in matters of healthy living and disease prevention, healthy diet.
In addition, the state sanitary-epidemiological situation may affect the following external factors:
- intensive epidemiological situation of the spread of dangerous infections in neighboring countries and the states of direct transport links with Kazakhstan;
- Kazakhstan's accession to the Customs
- Internal factors:
- lack of effectiveness of preventive examinations and early diagnosis;
- Inadequate implementation of new methods and protocols for diagnosis, treatment and rehabilitation of diseases, evidence-based medicine;
- Low-skilled professionals;
- Lack of continuity between primary care and
The state of the epidemiological situation and the effectiveness of the services affected by the following internal factors:
- Lack of service in the role of public health, including the prevention and reduction of disease com- municable diseases;
- Imperfect legal framework and organization of the service, the low level of harmonization with inter- national standards;
- Lack of effectiveness and efficiency of laboratory research services organizations;
- The low level of implementation of the activities of organizations of sanitary-epidemiological service, conducting laboratory research of modern innovative methods of work;
- Lack of implementation of the system of forecasting, risk management assessment in terms of optimi- zation and reduction of inspections of private enterprise;
- Low level of development of production base for the production of medical immunobiological prepa- rations, particularly diagnostics, test systems, etc. and strategic health development plan
In the health system, there are problems that are primarily related to the fact that the management and funding is focused on maintaining the capacity of the network, not on its effectiveness. Insufficient use of effective mechanisms (fund holding, two-capita standard) due to lack of funding for the incentive payments (44 %), imperfect legal framework, the lack of legal mechanisms (25 %), poor training of health care manag- ers (6 %).
Biased existing tariff system (not including depreciation), low autonomy of public health organizations and the lack of skilled managers significantly inhibit the development of competitive providers.
There is still an uneven distribution of resources across regions. So, in 2010, the cost of the spread GVFMA per inhabitant ranged from 12 964 to 21 289 tenge. GVFMA funding, despite the annual increase (from 64.8 bn in 2003 to $464.1 bln in 2010), also requires additional cost.
Remain problematic issues associated with a lack of logistical support of medical organizations. For example, emergency medical equipment medical equipment and medical supplies for the Republic of 51.69 %. In some regions of the country organizations providing medical care (ambulance station, primary care, forensics and others), are located in the non-standard, adapted buildings. 400 (4.3 %), health care organizations are located in unsafe buildings [3].
In addition, the limited development general practice in primary health care, and School health in preventive work with the population. Preserved unequal access to health services and poor quality of health services.
Despite the active implementation UHMIS, today remains a lack of information and communication infrastructure in the health sector, the low level of computer literacy among health workers, lack of automation of the process of health care, and adequate measures to optimize the number of beds, unnecessary hospitalizations and length of stay.
Rural health care in Kazakhstan is facing serious difficulties in isolation (distance), poor infrastructure, weak material base, adverse climatic conditions, lack of health care workers and staff turnover.
The difficulties encountered in the health care system associated with incorrect decisions made by officials in the instability of the market [Table 2].
The evolution of the Healthcare system for 2003 to 2011 [4]
T a b l e 2
![The evolution of the Healthcare system for 2003 to 2011 [4]](/uploads/data/files/pics8/2_232.jpg)
Source: Statistics Agency.
Тhe main indicators for the analysis of the effectiveness of health care is the growth of living standards. The growth of this index directly contacts to increase spending on health care. Policy of the state is connect- ed with increase in social spending, such as health, education and social security of vulnerable populations. Forecast and analysis carried out by analysis of indicators of contacts to these areas. Prediction of the state of health is now possible thanks to modern mathematical methods (regression and correlation.) We have studied the dependence of the number of health workers (V) of 7 factors for 2003–2011:
X1 — The number of physicians in all specialties, in thousands X2 — GDP, bln
X3 — Population, million people X4 — the average monthly salary X5 — The number of beds. Th.
X6 — Number of hospital organizations
X7 — Government outlays on health, million tenge
According to the statistics of factors for the period 2003 to 2011. calculated pair correlation coefficients presented in the form of a correlation matrix. We would like to note that the correlation table shows the close relationship between these factors, as the connecting factor of more than 0.9. However, the analysis also showed weak relationship between the factors x1 and x5, and a negative relationship between the factors of X3 and X6, X6 and X7 shows that spurious correlation, since these figures have close economic ties, such results can be explained by the policy of investing in the state health, as investments affect the performance in the long term, the trend growth related indicators is not an increase investment. In this regard, have been confiscation of factors with high correlation coefficients and thus have economic cohesion in the short term. To identify these factors, we have performed a re-analysis of indicators that’s matched in our requirements.
On the second correlation table revealed that there is a good correlation between the number of physi- cians in all specialties, in thousands (U) and average monthly salary (ryx4 = 0,92) and expenditure on health, U.S. tenge (ryx7 = 0,93). These factors have a direct impact on all specialty. Number of doctors may be justi- fied by the fact that statistics show an increase in the number of patients each year, and thus, there is a de- mand for seats in the House, and the state in turn increases the number of doctors. Just as the active policy of health, which leads to an increase in funding in the system.
For regression analysis, we chose the natural expression of the growth of these factors: the average monthly salary, n (x4) and expenditure on health, million tenge (x7).. If we consider the relationship of resultant of all the factors, then this problem, it should be noted that among the factors x4 and x7 is a good cor- relation between the factors and the strength of links, as the multiple correlation coefficient R = 0,90. Ac- cording to regression analysis 90 % of the variation in the number of doctors depends on the number of beds and expenditure on health (coefficient of determination R2 = 0,82). The resulting equation can be used to predict the health and prospects of the Republic of Kazakhstan, as the null hypothesis is rejected according to the random nature and recognized statistical significance and reliability of the regression model
(Ftabl = 4.74 <= Ffakt 11.9 ttabl = 2.36 <= 2.69 tv4; ttabl = 2.26 <= 5.59 tv7;). Multivariable regression equation for the growth rate is given by U = a + + b4h4 b7h7 = 52,7 +0,05 x4 +0.01 x7
Predictive value of Y is calculated for 10 and 11 periods separately, using polynomial function for fac- tors x4 and x7 (Figure).
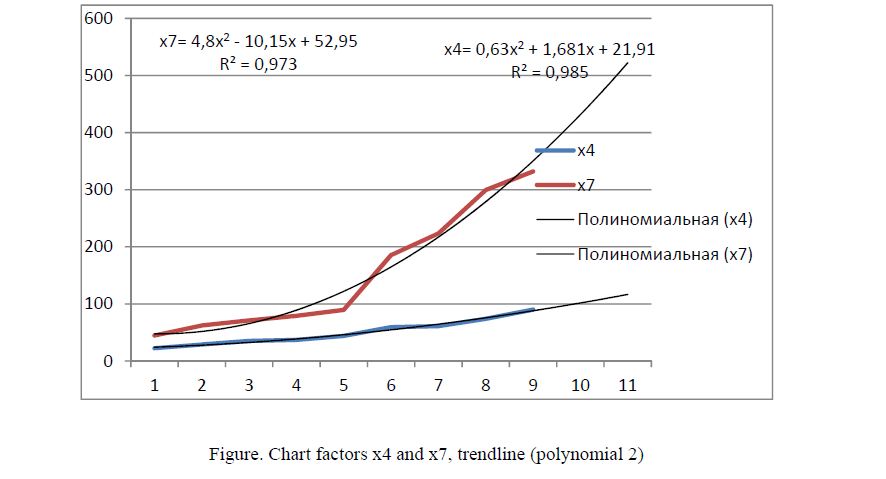
Figure. Chart factors x4 and x7, trendline (polynomial 2)
The initial data for 2003 to 2011. (9 periods) to construct time series for the factor number of beds, thousands (x4), we obtain the polynomial function of the form:
x4 = 0,63 x2 + 1,681 x + 21,91 R ² = 0,985, (t = 0,1,..., 9).
In this case, we find that the predictive value of x4 in 2012, when t = 10 is equal to 101.72 thousand tenge, forecast value for 2013 at t = 11 is equal to 116.631 thousand tenge. Followed by the initial data for 2003 and 2010. (9 periods) to construct time series for the factor of government expenditure on healthcare system (x7), we obtain the polynomial function of the form:
x7 = 4,8 x2 — 10,15 x + 52,95 R ² = 0,973 (t = 0,1,..., 9)
According to factor a polynomial function healthcare costs (x7), predictive value x7 in 2012 at t = 10 is equal to 431 million tenge, and the prognosis factor X7 in 2013 at t = 11 is equal to 522.1 mln.
The final part of the work we need to find the predicted values Y in real terms, and we find that the re- gression equation Y = a + I + b4h4 b7h7 = 52,7 +0,05 x4 +0.01 x7, forecast value for 2012 at t = 10 equal to 57.57 thousand, and in 2013 at t = 11 is equal to 57.72 thousand. In conclusion, we note that the analysis of the dynamics of the sector should analyzed by growth Y (%), and so the analysis showed that the number of physicians in the 10 and 11 period (2011–100 %) rose by 1.75, and also average monthly salary increased by times, which indicates a stable trend to
References
- State Program for Development of Health of the Republic of Kazakhstan for 2011–2015 «Salamatty »
- The Ministry of Health. Electronic resource — mz.gov.kz
- Health of the Republic of Kazakhstan and the organization of health in 2012 — Statistical Yearbook, National Centre for Health Development, Astana,
- Agency of Republic of Kazakhstan on Statistics. Electronic resource — stat.kz