Purpose of the research — to study the frequency of occurrence of polymorphism ST gene methylenetetrahydrofolate patients with diabetes mellitus type 2 and its correlation with homocysteine levels and the development of ischemic heart diseases. 118 patients with diabetes mellitus type 2 at the age of 45–60 years were surveyed. Statistically significant differences were observed frequencies of alleles of T and S, genotype SS between groups of patients with pancreatic diabetes type 2 with ischemic heart disease and transferred myocardial infarction and healthy persons. It was found that the allele T 677 gene, methylentetrahydrofolatreductase associated with an increased risk of myocardial infarction in patients with diabetes mellitus type 2 (OR=1,879, p=0,029). The combination of genotype T677 gene methylenetetrahydrofolatereductase with hyperhomocysteinemia in 2 type diabetic patients with coronary heart disease is related with other risk factors for cardiovascular diseases and can have a significant impact on the course of ischemic heart disease.
Аctuality of research. Cardiovascular diseases, in particular the coronary heart disease (CHD), are one of main cause of death of patients with diabetes (DM) [1]. The relative risk of its emergence is increased at men depended from age by 1,5–2,5 times, at women by 1,7–4 times and the increase in risk is always more expressed at women comparatively with men. Existence of DM is related with high risk of emergence of all ishemia forms (ICD), including stenocardy, ischemia of a myocardium, a myocardial infarct and death [2]. ICD in patients with DM in comparison with patients without DM develops at earlier age and characterized by more severe damage of coronary arteries with involvement of distal part [1, 2]. Pathogenesis of cardiovascular complications based on multiple factors and determined by insufficient metabolic control of DM, by immunological and hormonal changes as by changes in system of hemostasis. Previously a special significance in pathogenesis of the cardiovascular diseases (CD) is attached with genetic disorders [3, 4].
Now hard works on studying of one of genetic markers of CHD — polymorphism — of a gene 5,10 — a metylentetragidrofolatreductase (MTGFR) and its role in formation of this pathology are conducted. Polymorphism of a gene of MTGFR characterized by replacement of a cytosin on tymin in the T677th nucleotide (C677T) As result enzyme is transformed in thermolabile and its activity decrease by 30–65 %, that result destroying of processes of transformation of Homocysteine in Methionin and to development of a hypergomocysteinemya (HGC) [3, 5].
Recently value of HGC as important risk factor of atherosclerotic changes of vessels and also of arterial and venous tromboembolia is widely discussed [6–8]. Homocysteine (GC) is the sulfur-containing amino acid which is formed in the course of an exchange of methionine and cysteine. The methionine is metabolized with formation of S-adenosilhomocystein as result of hydrolysis, is transformed into GC. Disturbances of transformation of this amino acid into methionine and cysteine leads to increase in its content in blood. Increased GC level in plasma result activation of processes of oxidation with formation of free radicals toxic for endothelial cells that result proliferation muscle cells and stimulation of platelets and leukocytes [4, 9]. The HGC promotes oxidation of lipids that stimulates processes of atherogenesis [7, 8].
It was established that HGC high level in plasma of blood is independent risk factor for developing of CHD [4, 9]. It was showed that risk of cardiovascular pathology considerably increases when the CHD is combined with DM [6, 10, 11]. However there are MTGFR low studied polymorphism of a gene and its interrelation with the GC level and their influence on development of ICD at 2 type of DM.
Research objective. To study polymorphism of C677T of a gene of MTGFR, its interrelation with the GC level and role in development and progressing of ICD in patients with 2 type of DM.
Materials and methods
Genetic material was obtained from 118 patients with 2 type of DM aged from 45 till 60 years. Duration of disease is 7,8±5,7 years. For investigation influence of polymorphism gene of MTGFR on development of ICD patients were divided for 2 groups. The first group included 69 patients age — 53,6±4,4 years. This group in 42 patients in the anamnesis had a myocardial infarction (18 men and 24 women) age — 53,7±7,5 years. The second group 49 patients with 2 types of DM without ICD (15 men and 34 women), age — 52,1±4,3 years.
Criteria of exception from 1 and 2 groups: the age of patients till 45 years and over 60 years; existence at patients of chronic renal failure, recurrence of accompanying chronic diseases, of purulent — necrotic complication, B12-and folic acid deficiency induced anemia and also last month treatment by folic acid or vitamins of group B.
Control group included 89 patients (blood donors) aged from 45 till 60 years without disturbances of carbohydrate metabolism and the atherosclerosis and trombosis in the anamnesis.
All patient conducted full clinical and biochemical analysis. For identification of ICD Holterovsky monitoring of electrocardiogram using «Markett HELLIGE» system and a tredmillmetry using «HELLIGE CardioSoft V3.0» was carried out.
For DNA analysis samples of epithelial cells were used. Method phenolchloroformic extraction was used for separation of DNA. Polymorphic parts were amplifycated by Polymerase reaction using amplificator of «Eppendorf». Analysis of GC level was carried out by an immunoenzyme method using the analyzer IMMULITE 2000 type the Homocysteine (AXSIS) sets.
The statistical analysis was carried out using applied programs «Biostat» and «Statistica 6.0». All data are provided in a type of arithmetic averages and their standard deviation (M±SD). Tests for balance of Hardy — Weinberg and identification of associations by method χ2. Reliability of coefficients of distinctions was accepted at value р<0,05. For estimation of associations of polymorphic options with pathological phenotype a relative risk (OR — odds ratio) was counted using formula OR = ad/bc, where: a — frequency analyzed allele at patients; b — frequency analyzed allele in control selection; c and d — total frequency of other alleles at patients and in control respectively. The size OR = 1 indicated absence of association at OR>1 the positive association allele with a disease («risk factor») were confirmed, at OR<1 — negative association allele with disease, as protective action given allele.
Results and discussion
Results demonstrated prevalence of normal alleles C677 in patients with type 2 of DM which was defined at 75,4 % of patients. Thus an allele of T677 which in some researches proved as a marker of CHD [12, 13] was revealed at 24,6 % of patients and at 21,9 % of persons of control group (OR=1,161, C.I. = [0,731–1,844], χ² = 0,40, p=0,52) (Table 1).
Frequency of alleles and genotypes of C677T polymorphic locus of MTHFR gene in patients with type 2 diabetes mellitus and in the control group
T a b l e 1
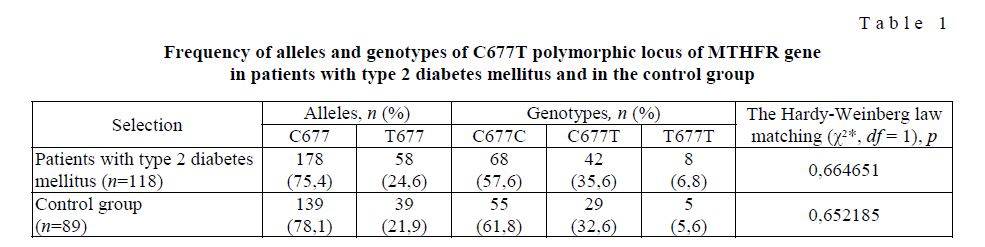
Frequency of occurrence of genotypes corresponded to Hardy's law — Weinberg (table 1). At the surveyed patients with 2 type of DM the heterozygotic genotype of C677T showed in 35,6 % of cases; the homozygous (normal) genotype of C677C — in 57,6 %; at 6,8 % of patients was a homozygous genotype of T677T.
Statistically significant distinction in frequencies of occurrence of genotypes of C677C, C677T and T677T between patients with 2 type of DM and control group is not revealed (table 1). At calculation of stratification risk the DM it was revealed some association of 2 types with T677 alleles (to OR = 1,1) with homozygous genotype of T677T (OR = 1,2) and with heterozygotic genotype of C677T (OR = 1,1) but this association wasn't reliable. There are risk for developing of ICD in patients with a homozygous genotype of T677T [9, 10].
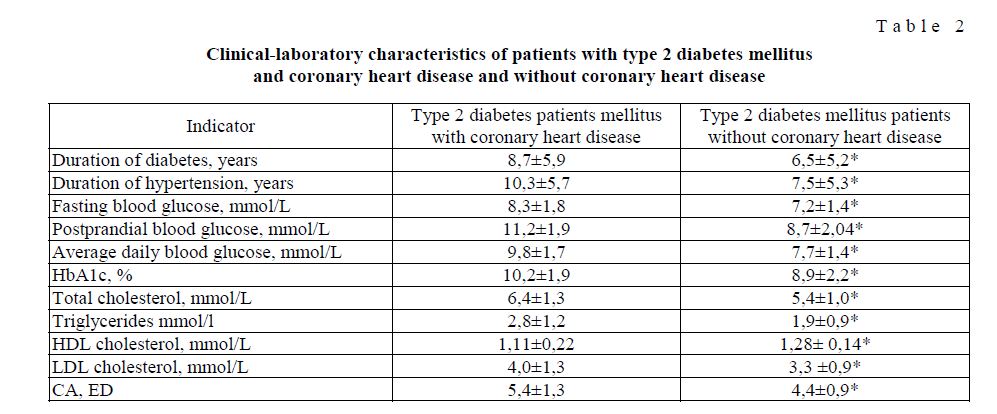
One of problems of this research was to estimate influence of polymorphism of a gene of MTGFR as one of the factors of influence on metabolism of a homocystein on development of ICD. Results of investigation patients with IСВ duration of current of DM and of arterial hypertension (AH), glycemia before and postprandial were authentically higher as more high level of HbA1c. In patients with ICD a higher level of cholesterol (OHS), triglycerides (TG), lipoproteides of the low density (LPNP) and the lowered indicators of lipoproteides of the high density (LPVP) (table 2) are registered. These results correspond to data obtained by other authors [1, 14].
A.Engbersen et al. [15], A.Gardemann et al. [16] demonstrated existence of association of a homozygous genotype of T677T of gene of MTGFR with CHD [13, 11]. Other researchers didn't find relation between this polymorphism and vascular pathology [5, 17].
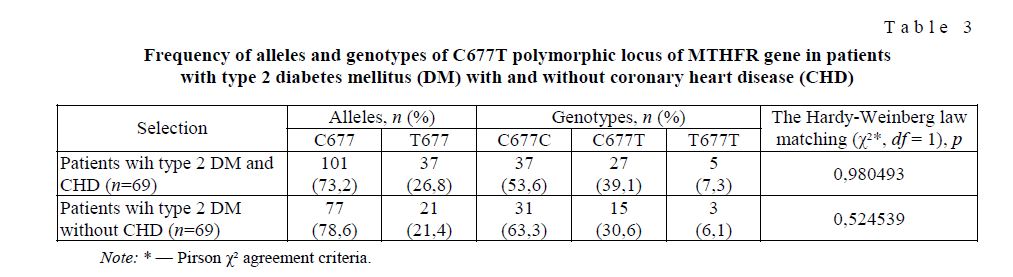
Results demonstrated that frequency of allele Т677 of gene MTGFR in patients with DM 2 types with ICD and without ICD authentically didn't differ in gene MTGFR at patients with DM and made 26,8 % and 21,4 % respectively (table 3).
Analysis of distribution of genotypes of MTGFR at 7,3 % of patients with 2 type DM with ICD and at 6,1 % of patients without ICD are revealed existence of a homozygous (T677T) genotype of MTGFR (table 3). The heterozygot genotype of C677T prevailed in patients of 1 group (2 type DM with IBS) in compared with patients of 2 groups (2 type DM without IBS) (39,1 % and 30,6 %, respectively. Analysis of stratification risk the DM showed some association 2 types in combination with ICD with T677 alleles (to OR = 1,3), a homozygous genotype of T677T is revealed (OR = 1,4) and a heterozygotic genotype of C677T (OR = 1,3). However this association isn't reliable. Similar data are described also by other authors. In groups of the French, Swedish and Australian patients with CHD the association of allele T677 and a genotype of T677T of a gene of MTGFR with atherosclerotic damage of coronary arteries is also not revealed [11, 12, 18].
Clinical-laboratory characteristics of patients with type 2 diabetes mellitus and coronary heart disease and without coronary heart disease
T a b l e 2
T a b l e 3
Frequency of alleles and genotypes of C677T polymorphic locus of MTHFR gene in patients with type 2 diabetes mellitus (DM) with and without coronary heart disease (CHD)
It was demonstrated the presence of high frequency of allele by T677 in patients with repeated myocardial infarctions and correlation this allele with the HZ level in serum [10, 19, 20]. A.Gardemann et al., 1999, demonstrated polymorphism of C677T of MTGFR almost at 2500 Europeans with angiographic the verified atherosclerosis of coronary arteries was investigated. It was noted that carriers of a homozygous genotype of T677T have higher rate of atherosclerotic damage of coronary arteries comparatively with patients have as least one allele of C677 [16].
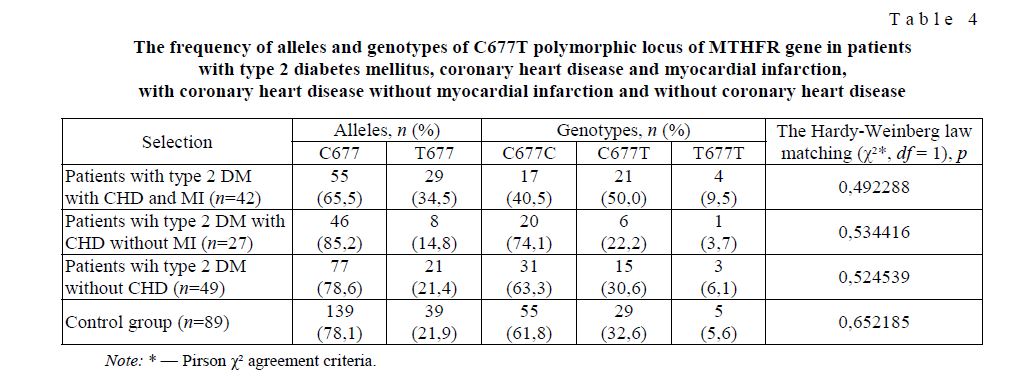
This regard on the analysis of polymorphism of gene MTGFR in patients with 2 type of DM with ICD depending of existence or absence in anamnesis of a myocardial infarction was carried out. Patients with 2 type of DM with a myocardial infarction in the anamnesis differed from control group on the frequency of occurrence of alleles of T677 (OR=1,879, C.I. [1,059–3,333], χ ²= 4,72, p=0,029) and C677 (OR= 0,532, C.I.
[0,300–0,944], χ² = 4,72, p=0,029). At patients past myocardial infarction less than in control the homozygous genotype of C677C (OR=0,420, C.I was observed. [0,199–0,890], χ²=5,24, p=0,022). Also high frequency of genotypes of C677T and T677T (50 % and 9,5 %, respectively) in this group of patients is found in comparison with control group (32,6 % and 5,6 %, respectively) but this distinction wasn't reliable (table 4). Carriers of allele T677 had increased risk of development of a myocardial infarction (OR=1,879, C.I. [1,059–3,333], χ ² = 4,72, r=0,029).
Patients with myocardial infarction in anamnesis differed on frequency of occurrence of polymorphism of a gene MTGFR not only from healthy people but also from patients with 2 type of DM without ICD and with ICD but without myocardial infarction. Allele of T677 I is found at 34,5 % of patients with myocardial infarction whereas at patients without myocardial infarction and without ICD was revealed at 14,8 % and 21,4 %, respectively (χ ² =7,78, r=0,02) (table 4). In group of patients with 2 type of DM and myocardial infarction are revealed prevalence of heterozygotic C677T (χ²=6,43, r=0,04) and homozygous T677T (χ²=0,93, r=0,62) genotype in compared with patients with 2 type of DM with ICD without myocardial infarction and 2 types DM without IBS (table 4).
T a b l e 4
The frequency of alleles and genotypes of C677T polymorphic locus of MTHFR gene in patients with type 2 diabetes mellitus, coronary heart disease and myocardial infarction, with coronary heart disease without myocardial infarction and without coronary heart disease
It is known that polymorphism of gene MTGFR can be one of the cause of the HZ causing increase. In patients with 2 type of DM were found higher values of HZ than at persons of control group: 14,0±5,2 umol/l in patients with 2 type of DM and ICD (rk=0,001); 11,6±4,8 umol/l in patients with 2 type of DM without IBS and 9,38±5,4 umol/l in control (Fig.1).
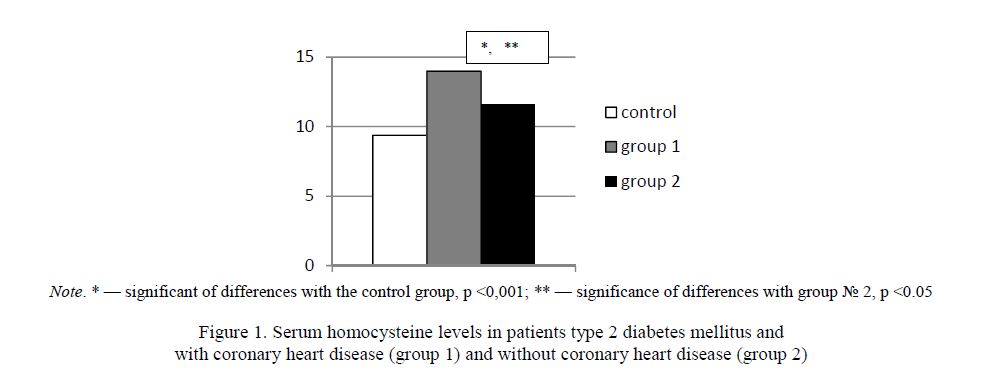
Figure 1. Serum homocysteine levels in patients type 2 diabetes mellitus and with coronary heart disease (group 1) and without coronary heart disease (group 2)
The average level of HZ at patients with the postponed myocardial infarction was authentically higher in comparison with patients without myocardial infarction (15,3±4,3 and 12,1±5,4 of umol/l respectively, p<0,05) (Fig. 2).
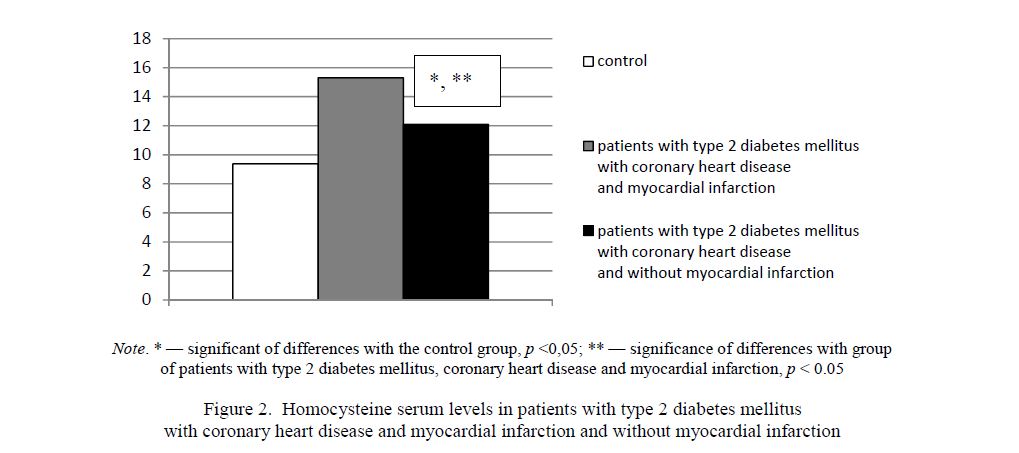
Figure 2. Homocysteine serum levels in patients with type 2 diabetes mellitus with coronary heart disease and myocardial infarction and without myocardial infarction
Analysis of results of research HZ depending of polymorphism of a gene MTGFR showed that both in control and at patients with 2 type of DM (in 1 and 2 groups) the HZ greatest level is revealed at a homozygous genotype of T677T (Table 5). Especially it was observed in patients with a myocardial infarction in the anamnesis where at a homozygous and heterozygotic genotype of T677T and C677T the greatest values of HZ (Table 6) are revealed. Similar results were showed by K.Arai et al. (1997) that the level of a gomocysteinemiya is higher in patients with 2 type of DM with T677T MTGFR gene genotype than at surveyed with C677C a genotype. Also in group of patients with 2 type of DM with T677T the genotype revealed the high frequency of a myocardial infarction.
C677T polymorphism of MTHFR gene and serum homocysteine levels in patients with type 2 diabetes mellitus and in the control group
T a b l e 5
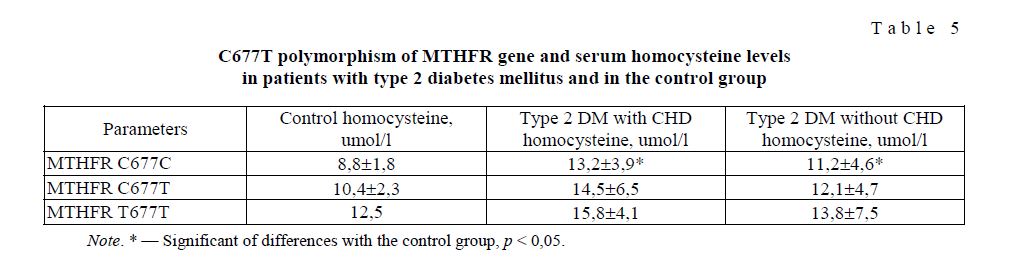
Thus, authors showed that T677T MTGFR gene genotype indirectly, through moderated by GHZ stimulated developing of atherosclerosis in patients with 2 type of DM and increases risk of a myocardial infarction [6].
Multiple-factor regression analysis of the HZ level in patients with 2 type of DM with ICD with myocardial infarction in the anamnesis and a homozygous genotype of T677T with other risk factors of ICD where in model as independent factor are a variables duration of DM and AG, level of systolic and diastolic the blood pressure, a glycemia before and postprandial, OHS, TG, LPVP, LPNP and as the dependent factor — the level of HZ, showed that HZ level at patients with a homozygous genotype of T677T depended of level of a preand postprandial glycemia as of daily glycemia and of HbA1c, LPVP, TG (R2 = 0,99; r = 0,014).
T a b l e 6
C677T polymorphism of gene MTHFR and homocysteine serum levels in patients with type 2 diabetes mellitus and coronary heart disease and myocardial infarction and without myocardial infarction
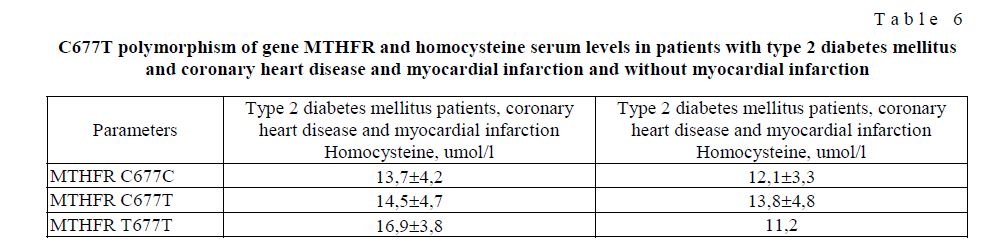
Thus, a high HZ level at a homozygous genotype of T677T of a gene of MTGFR can be an important factor in development of a myocardial infarction in patients with 2 type of DM.
Conclusions:
- Frequency of occurrence of alleles and genotypes of C677T of a gene of MTGFR at patients with 2 type of diabetes without and with Ishemical Cardiac Disease (ICD) but without myocardial infarction in the anamnesis corresponded to control
- Patients with 2 type of diabetes with a myocardial infarction in anamnesis differed from control group on the frequency of occurrence of alleles of T677 and C677 of gene of MTGFR (r=0,029). An allele of T677 of gene of MTGFR have relation with the increased risk of development of myocardial infarction patients with 2 type of diabetes (OR=1,879, r=0,029).
- In patients with 2 type of diabetes ICD the HZ high level of serum of blood revealed in comparison with patients without ICD and control
- Combination of homozygous genotype of T677T of gene of MTGFR to GHZ in patients with type 2 of DM with ICD and a myocardial infarction in the anamnesis is related with other risk factors of cardiovascular diseases (level of a preand post-prandial glycemia, average daily glycemia, HbA1c, LPVP, TG and can have important influense on current of ICD and myocardial
References
- Alexandrov A.A. Consilium medicum, 2001, 10, p. 464–468.
- Betteridge D.J. Medicographia, 2001, 23, p. 95–99.
- Rams V.S., Aseev M.V., Baranova E.V. Nature, 1999, 3, p. 5–8.
- Kotelnikov M.V. Cardiology, 2004, 10, p. 102–106.
- Spiridonova M.G., Stepanov V.A., Puzyrev V.P. Clinical medicine, 2001, 2, p. 11–16.
- Hoogeveen E.K., Kostense P.J., Jakobs C. Circulation, 2000, 5, p. 1506–1511.
- Loscalzo J. Clin. Invest., 1996, 98, 1, p. 5–7.
- Wotherspoon F., Laight D., Shaw K., Cummings M. J. Diabetes Vasc. Dis., 2003, 3, p. 334–340.
- Hubutiya M.Sh., Shevchenko O.P. Gomotsistein at a coronary heart trouble and a warm transplantant, Moscow: Reafarm, 2004, 271
- Jeremy J.J., Shukba N., Angelini G.D. Atherosclerosis, 2002, 164, p. 383–384.
- Passaro A., D’Elia H., Pareschi D. et al. Diabetes Care, 2000, 23, 3, p. 420–421.
- Arai , Jamasaki J., Kajimoto J., Watada H., Umayahara J., Kodama M., Sakomoto K., Hori M. Diabetes, 1997, 12, P. 2102–2104.
- Brattstrom L., Wilcken D., Whrvik J., Brudin L. Circulation, 1998, 98, p. 2520–2526.
- Turner R., Millns H., Neil H. et al. BMJ, 1998, 316, p. 823–828.
- Engbersen A., Franken D., Boers G. et al. J. Hum. Genet., 1995, 56, p. 142–150.
- Gardemann A., Weidemann H., Philipp M. et al. Heart. J., 1999, 20, p.584–592.
- Brulhart M.-C., Dussoix Ph., Puiz J. et al. J. Hum. Genet., 1997, 60, p. 228–229.
- Wilcken D., Wang X., Sim A., McCredie R. Arteriosclerosis Thrombos. Vasc. Biol., 1996, 16, p. 878–882.
- Kluijtmans L., van den Heuvel L., Boers G. et al. Atherosclerosis, 1998, 43, p. 414–421.
- Morita H., Kurihara H., Tsubaki S. et al. Thrombos. Vasc. Biol., 1998, 18, p. 1465–1469.