We have investigated 20 patients with type 2 diabetes, with an average age of 58,0 ± 4,32 years, with disease duration of 6,29 ± 1,28 years. The carbohydrate metabolism was estimated: fasting blood glucose and 2 hours later after meal, glycosylated hemoglobin (HbA1C). For the purpose of determine the safety of insulin analogues, have been studied biochemical parameters of blood before and after 3 months of therapy. The basic criterion of the safety of the therapy within 3 months of application study of insulin analogues was the number of daytime and nighttime hypoglycaemia, as well as the dynamics of body weight during the study period. Structural and functional state of the left parts of heart was assessed by echocardiography and dopplerography of transmitral blood flow. For all patients were assigned insulin analogues, the average daily dose was 32,4 ± 2,8 units, particularly rapid-acting insulin aspart (Novorapid) and acting insulin detemir (Levemir). Analogs of human insulin had a favorable effect on carbohydrate metabolism and reduced the incidence of nocturnal hypoglycemia. Also, there was a trend to improvement of the structural parameters and left ventricular diastolic function in patients with type 2 diabetes after treatment with insulin analogues. Application of insulin analogues have proven the safety of the insulin group in terms of prevention of hypoglycemia, which has a positive effect on cardiovascular events in the outcome of the treatment of diabetes.
The problem of diabetes mellitus (DM) has become «pandemic», and the number of patients as per the IDF Diabetes Atlas (2012) is 366 million (6.6 %). According to the expert forecast, that number of the patients with diabetes can raise up to 552 million (8 %) by 2030. In-growth is going to occur almost exclusively at the expense of patients with the type 2 diabetes mellitus in both developed countries and the developing countries [1, 2]. In 2010, in the Republic of Uzbekistan there were 117,240 (0.45 %) patients with diabetes mellitus registered; however, the results of epidemiological studies showed that in fact the number of patients was 10 times higher [3]. The large social significance of diabetes is that it leads to early disability and mortality at the expense of late vascular complications.
There are two underlying endocrine defects in the pathogenesis of this disease: impaired insulin production and peripheral insulin resistance. It is the insulin resistance which causes the excessive hepatic glucose production manifested, in particular, by morning hyperglycemia [4]. Hyperglycemia is an independent risk factor for late macroand micro vascular complications in type 2 diabetes mellitus, as well as one of the major risk factors for mortality in cardiovascular diseases [5, 6].
Given the scale of developing epidemic of DM there is an urgent need to develop an effective therapeutic algorithm of blood-glucose-lowering treatment, which allows achieving the compensation of carbohydrate metabolism and preventing the development of severe vascular complications of this disease. At that, the efficacy of blood-glucose-lowering action of drugs concomitantly with their safety (both short-and longterm) for patients should be the priority in the selection of therapeutic agents. The presence of severe complications of DM, especially, of cardiovascular ones, imposes certain restrictions on setting individual goals of glycemic control. The results of studies such as ACCORD, VADT, ADVANCE and UKPDS (which also involved Russian endocrinology and cardiology centers), show that in the presence of cardiovascular complications the achievement of normoglycemia is dangerous due to the development of hypoglycemia resulting in cardio-cerebrovascular outcomes [7].
The chronic, relentlessly progressive nature of the type 2 diabetes course inevitably leads to the fact that sooner or later most patients with diabetes are unable to achieve or maintain an optimal long-term glycemic control with the help of diet therapy and medications (oral blood-glucose-lowering drugs) [8, 9]. The retrospective analysis of the UKPDS shows that about 50 % of B-cells in the pancreas have been destroyed and have lost their function by the time of the diagnosis of the type 2 diabetes [10]. With the development of the disease, the function of remaining B-cells in the pancreas becomes worse and, therefore the majority of patients require an adequate blood-glucose-lowering therapy [11]. However, within six years from the time of the diagnosis, as the disease progresses, most patients need an insulin therapy [12].
Over the past decade, the treatment approaches have changed. The importance of an individualized approach is increasing. Regardless of the age at which the diagnosis is established, DM is a lifelong disease, and the patients should follow the particulars of the treatment. Current data indicate the existence of the effect of «metabolic memory» whereby even short periods of poor glycemic control at the onset of the disease may increase the risk of future complications and long-term adverse outcomes, especially in respect of the cardiovascular system [13, 14]. Other studies emphasize the negative impact of hypoglycemia caused by an intensive insulin therapy on the cardiovascular system and mortality of patients with the type 2 DM. This issue remains unresolved; the available data are contradictory and not clear [7]. The individualized therapeutic approach recommended today in diabetes mellitus implies an optimal balance of the efficacy and risk of adverse events for each patient [15].
The type 2 diabetes is a progressive disease. The stage of insulin hypersecretion is replaced by the stage of «exhaustion»; during this period, an insulin deficiency occurs, and the patient begins to need an insulin therapy. Different types of insulin are used for the initiation of an insulin therapy and its further intensification. More than 80 years have passed since insulin was discovered. The first commercial insulin preparations were far from ideal, however, the rapid improvement in the technology led to the appearance of highly purified animal insulins, long-acting insulins, and finally, the recombinant human insulin. The completion of the DCCT and UKPDS studies, which demonstrated the ability to prevent the development and progression of diabetic complications with the tight glycemic control, was an important event for diabetology. At the same time, the shortcomings of standard insulin preparations, which did not provide the required flexibility of the therapy and often caused hypoglycemia when trying to normalize the level of HbA1c, became apparent. Today, modern genetic engineering technologies allow making changes to the structure of recombinant protein molecules and getting modified insulins (analogues). The first decade of the XXI century was an epoch of the rapid and widespread introduction of insulin analogues, as the most physiologic and effective drugs to replace a relative and absolute insulin deficiency [16, 3].
The reasons of poor compensation of the type 2 diabetes are varied, and not least related to economic factors, the organization of health care, etc. However, the special barriers to an effective therapy of diabetes are caused by the peculiarities of the perception of the treatment process by both patients and medical personnel. There is a «psychological insulin resistance» to a pathogenetically associated insulin therapy in the type 2 diabetes, not only in the patients but also in doctors. This situation often leads to a late prescription of insulin on the background of the progressive course of the disease and formed severe complications of diabetes, when it is impossible to significantly improve the prognosis. The phenomenon of «clinical inertia» (the delayed start and intensification of insulin therapy) is now well-known and experts define it primarily as a medical problem [8]. Naturally, for the doctor, there are many quite rational concerns about the prescription and treatment with insulin, especially concerns regarding hypoglycemia and weight gain. However, these adverse events are actually a natural consequence of the effective action of insulin. It is impossible to completely get rid of them, and the minimization of these effects is the most important task. It is not allowed to neglect the achievement of compensation trying to avoid adverse events [8]. The selection of insulin preparations with least side effects, a simple mode of administration and available algorithms of the dose titration is one of the most effective ways to prevent both clinical inertia and psychological insulin resistance. On that score, the insulin analogues that have recently been introduced into the wide clinical practice for the treatment of DM are preferable. Every year, these preparations become widely popular among both doctors and patients. This is due to their high efficacy, good safety profile and physiological insulin secretion. The clinical efficacy of insulin analogues is determined by the following criteria: the binding to insulin receptors in target tissues, the metabolic / mitogenic potency ratio, biochemical and physical activity and immunogenicity. One of the preparations for the treatment of DM is Detemir (the trade name is Levemir), which is classified among acylated long-acting recombinant human insulin analogues. The results of pharmacodynamic studies have shown that detemir has a more predictable blood-glucose-lowering effect than other basal insulins. The results of several international clinical trials have convincingly shown that the use of Levemir is safe and effective in the patients with type 2 diabetes at the initiation of insulin therapy as a single agent and in combination with oral blood-glucose-lowering agents [9].
The combination of basal and rapid-acting insulin analogues creates a more physiologic profile of action than the regular human insulin, and it is used to improve the efficacy and tolerability.
The information on the effect of insulin on the cardiovascular system in type 2 diabetes is very contradictory. Despite the fact that an insulin therapy is considered the standard for glycemic control in high insulin resistance, the use of insulin is not always beneficial for patients with cardiovascular diseases because of the possible development of hypoglycemia [4, 17–20]. However, the results of numerous randomized clinical trials indicate that a significant improvement of glycemic control under the therapy with insulin analogues is associated with a very low incidence of severe and nocturnal hypoglycemia and almost no risk of severe hypoglycemia in the monotherapy with Levemir® insulin. What is one of the measures to prevent the progression of cardiovascular diseases in people with type 2 diabetes? In light of the facts above, we decided to evaluate the effect of insulin analogues on both carbohydrate metabolism and structural-functional parameters of the cardiovascular system in the patients with type 2 diabetes.
The aim of the study was to investigate the effect of insulin analogues on the diastolic dysfunction and structural-functional parameters of the left ventricular myocardium in the patients with type 2 diabetes.
Material and methods. The study included 20 patients with moderate type 2 diabetes, the average age of 58.0 ± 4.32 years, disease duration of 6.29 ± 1.28 years, who received inpatient treatment in the endocrinology department of clinic No.3 of Tashkent Medical Academy. The degree of compensation of carbohydrate metabolism was evaluated taking into account the fasting blood glucose levels and the blood glucose levels in 2 hours after a meal, as well as by determining the glycosylated hemoglobin level (HbA1C). In order to determine the safety of insulin analogues, the levels of ALT, AST, creatinine, blood urea were investigated before the therapy and after 3 months of the therapy. The number of diurnal and nocturnal hypoglycemic states within 3 months of using the studied insulin analogues, as well as the dynamics of the body weight change during the period of the study was the main criterion of the safety of the therapy conducted. All the patients were assigned to insulin analogues, namely, aspart (NovoRapid) — an ultrashort-acting insulin and detemir (Levemir) — prolonged-acting insulin, at an average daily dose of 32.4 ± 2.8 units.
The structural-functional state of the left parts of the heart was assessed by the echocardiography and Doppler ultrasound of the transmitral blood flow [21–24, 15]. The investigation was conducted at Sonos ultrasonic cardiograph produced in the USA, with the dopplerographic attachment. The structural parameters of the heart were determined during the investigation in the one-dimensional mode. The pulsed Doppler EchoCG was conducted using B-mode EchoCG [25]. The transmitral blood flow was recorded from the apical 5or 4-chamber view. The left atrial (LA) end-diastolic dimension and left ventricular end-diastolic dimension, the thickness (mm) of the left ventricular posterior wall (LVPW) and interventricular septum (IVS) in diastole, left ventricular end-diastolic volume (LV EDV, ml), left ventricular ejection fraction (LVEF, %) were determined in the echocardiography [5]. The left ventricular mass (LVM, g) was determined by the formula of Devereux R., Reichek N. (1977); the left ventricular mass index (LVMI, g/m2): the LVM / body surface area ratio (Devereux R., 1984); left ventricular relative wall thickness index (LV RWTI, mm): the sum of the thickness of LVPW and IVS / LV EDD ratio. The transmitral diastolic flow was investigated to assess the left ventricular diastolic function: the peak of the LV rapid diastolic filling (VЕ, m/sec.) / peak of active atrial filling (VА, m/sec.) ratio — VЕ/VA or Е/А.This study of the patients with type 2 diabetes was carried out before the treatment and after 3 months of the treatment with the insulin analogues.
Results. The analysis of changes in the measures of carbohydrate metabolism, body mass index (BMI), and a daily dose of insulin after 3 months of insulin therapy, was performed (Table 1).
T a b l e 1
The analysis of changes in the measures of carbohydrate metabolism, body mass index (BMI), and a daily dose of insulin after 3 months of insulin therapy
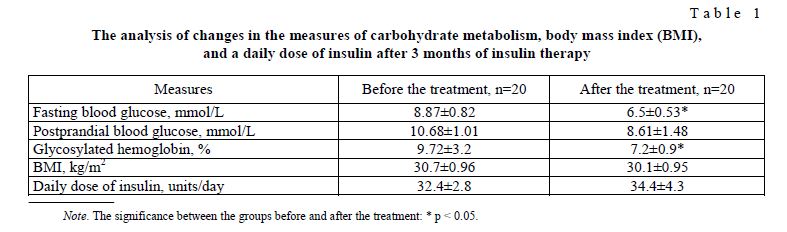
The measures of carbohydrate metabolism, such as, fasting blood glucose, postprandial blood glucose, glycosylated hemoglobin after the insulin therapy decreased by 26.7 %, 19.4 %, 25.9 % respectively. Under the treatment with insulin analogues, the body mass index (BMI) remained unaltered. The daily dose increased by 6.2 % taking into account the titration of insulin.
The levels of ALT, AST, creatinine, and blood urea were measured before and after the administration to determine the effect of the insulin analogues on the liver and kidney functions (Table 2).
Measures of liver and kidney functions under the therapy with the insulin analogues
T a b l e 2
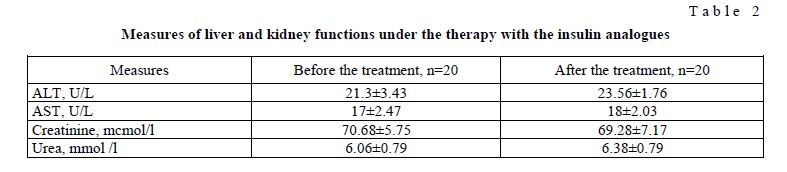
According to the findings of the study, no significant effect on the liver and kidney functions was found.
The incidence of hypoglycemic states is an independent measure of the safety of the replacement insulin therapy conducted (Table 3).
The incidence of hypoglycemic states
T a b l e 3

Based on the anamnestic data it was found that after 3 months, under the intensive metabolic control of the disease, there is a slight decrease in the incidence of diurnal hypoglycemia. Meanwhile, it was a very significant fact that the incidence of the nocturnal hypoglycemia decreased by almost 2 times; it was 13.5 % versus 29.3 %, which was primarily due to the positive pharmacodynamic properties of the insulin analogues.
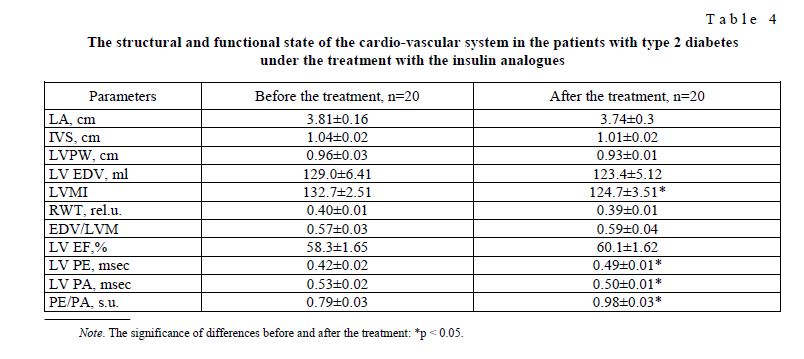
There was a trend towards the improvement of the left ventricular structural parameters and diastolic function in the patients with type 2 diabetes after the treatment with the insulin analogues. The following changes were observed: the left atrial diameter decreased by 1.9 % and the left ventricular end-diastolic volume (LV EDV) — by 4.4 %; the thickness of the interventricular septum (IVS) was reduced by 2.9 % and the left ventricular posterior wall (LVPW) — by 3.24 % and the relative wall thickness (RWT) — by 1.8 %. The reduction of the wall thickness and internal volume of the cavity of the left ventricle resulted in the decrease in the left ventricular mass index (LVMI) by 6.1 %. In investigating the LV diastolic function, the significant increase in the PE by16.4 % and the decrease in the PA by 5.7 % were found, as well as the increase in the E / A ratio by 24 %; that is the evidence of the improved diastolic function.
The LV structure and diastolic function changed under the treatment with the insulin analogues (Table 4).
T a b l e 4
The structural and functional state of the cardio-vascular system in the patients with type 2 diabetes under the treatment with the insulin analogues
Discussion. Thus, according to our study, the efficacy and safety of human insulin analogues when used in the patients with the type 2 diabetes, were proved, as well as the trend towards the improvement of the left ventricular structural parameters and diastolic function was observed.
According to Veterans Affairs Diabetes Trial (VADT), it was found that pronounced hypoglycemic reactions in the type 2 DM were the main predictors of myocardial infarction, stroke and death from all causes [26]. The maintenance of the compensation of DM providing a НbА1с level of less than 6.5 % was the starting point for planning the large-scale multicenter randomized two-factor study — ACCORD (Action to Control Cardiovascular Risk in Diabetes), as the primary role of hyperglycemia in the pathogenesis of angiopathy proceeding with the affection of both small and large vessels was proved. When analyzing the overall mortality rate it was observed that in the total group of patients with type 2 diabetes, in patients without hypoglycemic episodes it was 1.2 % per year, and in the presence of hypoglycemia — 3.3 % per year. Moreover, in both branches of the study, the mortality was higher in subgroups with recorded hypoglycemic episodes (2.8 vs. 1.3 % per year in the intensive-control group and 4.9 % versus 1.1 % per year in the standard –control group). Thus, the mortality was higher in the patients with recorded hypoglycemic episodes regardless of a therapeutic strategy. In the risk assessment it was determined that the risk of death was higher in the group of intensive hypoglycemic therapy, in individuals without recorded hypoglycemic episodes, whereas in the group of standard therapy, the mortality was highest in the patients with recorded hypoglycemia.
It was concluded that it is hypoglycemia that causes an increase in the risk of negative cardiac outcomes.
The relative risk of myocardial infarction (MI) associated with undergone episodes of severe hypoglycemia 1 year before MI is 12 %, 5.5 months before MI is 20 %, 2 weeks before MI is 65 % [27].
The consensus the ADA and the scientific analysis of the American College of Cardiology and the American Heart Association: severe hypoglycemia is considered as the most likely reason for the increase in the cardiovascular mortality in the group of intensive glycemic control [27].
The death from hypoglycemia may be mistaken for the death from acute coronary syndrome, as it is generally not preceded by the measurement of the blood glucose level. Anatomical and morphological postmortem signs of hypoglycemia are absent.
Despite the fact that the results may indicate that the decrease in the blood glucose levels to the average НbА1с level of 6.5 % s as a result of the treatment does not reduce the risk of macrovascular events, these data do not detract from the benefit which can be derived as a result of the obtained significant difference between the groups of intensive and standard controls in reducing the risk of total events — serious macro — and microvascular events in the group of intensive therapy.
Thus, hypoglycemic episodes have a negative impact on the course of DM, not only from the standpoint of the difficulties in achieving the compensation, but cause an increased risk of acute cardiovascular events. Cardiovascular events increase the probability of death, cause difficulties in providing the compensation for diabetes and initiate the development of microvascular complications also resulting in a negative prognosis [28].
Our findings in respect of the effect of the insulin analogues on the structural-functional parameters once again proved the safety of this insulin group in terms of the prevention of hypoglycemia, and that has a positive effect on the cardiovascular events in the treatment outcome of diabetes.
Conclusions:
- The human insulin analogues had a beneficial effect on the carbohydrate metabolism: significantly reduced the fasting glucose, postprandial blood glucose, led to the reduction of glycosylated hemoglobin compared to the baseline values by 25.9 %, which certainly indicates a high clinical efficacy of insulin analogues in the treatment of
- No effect on the liver and kidney functions in the application of the insulin analogues was
- The application of insulin analogues in the treatment of type 2 diabetes mellitus helped to reduce the incidence of nocturnal hypoglycemia by 15.3 %.
- There was a trend towards the improvement of the left ventricular structural parameters and diastolic function in the patients with the type 2 diabetes after the treatment with the insulin analogues: the left atrial diameter decreased by 9 %, the LV EDV — by 4.4 %; the IVS was reduced by 2.9 %, the LVPW — by 3.24 %, the RWT — by 1.8 %, the LVMI — by 6.1 %; the increase in the PE was by16.4 %, the decrease in the PA — by 5.7 %, the increase in the E / A ratio — by 24 %; that is the evidence of the trend towards the improved diastolic function.
- The application of the insulin analogues proved the safety of this group of insulins in terms of the prevention of hypoglycemia, and that has a positive effect on cardiovascular events in the treatment outcome of diabetes.
References
- American Diabetes Association. Diabetes Care, 2007, 30, 1, p. S4–S41.
- Global Guideline for Type 2 Diabetes; IDF,
- Akbarov S., Ismoilov S.I., Alikhanova N.M., Kayumova D.T., Rakhimzhanova M.T., Kasymov U.A., Normatova N.M. Journal of theoretical and clinical medicine, Tashkent, 2012, 6, p. 39–42.
- Antsiferov M.B., Dorofeyeva L.G., Petraneva E.V. Farmateka, Moscow, 2005, 107, 12, p. 24–29.
- Khaw T., Wareham N., Bingham S., Luben R., Welch A., Day N. Ann. Intern. Med., 2004, Sep. 21, 141(6), p. 413–420.
- World Health Organization, World Heart Federation, World Stroke Organization. [Accessed April 1, 2013]; Global atlas on cardiovascular disease prevention and control, 2011, p. 1–164.
- Dedov I.I., Shestakova M.V., Ametov A.S., Antsiferov M.B., Galstyan G.R., Majorov A.Yu. Diabetes, Moscow, 2011, 4. — 98–99.
- Riedel A.A., Heien H., Wogen G., Plauschinat C.A. Pharmacotherapy, 2007, Aug., 27(8), p. 1102–1110.
- UK Prospective Diabetes Study (UKPDS) Group. Lancet, 1998 Sep 12, 352(9131), p. 837–853.
- Lebovitz E. Diabetes Rev., 1999, 7, p. 139–153 (data are from the UKPDS population: UKPDS 16, Diabetes, 1995, 44, р. 1249–1258.
- Mariëlle J.P. van Avendonk and Guy E.H., Rutten M. Diabetes, Obesity and Metabolism, 2009, 11(5), p. 415–432.
- Wright A., Burden A.C., Paisey R.B., Cull C.A., Holman R.R. Diabetes Care, 2002, Jul., 25(7), p.
- Chaturvedi N. Circulation, 2009, 119, p. 2886–2893.
- Holman R.R., Paul S.K., Bethel M.A., Matthews D.R., Neil H.A. Engl. G. Med., 2008, 359, p. 1577–1589.
- Surkovа E.V. Diabetes, Moscow, 2013, 1, p. 52–54.
- Hermansen K., Davies M., Derezinski T. Diabetes Care, 2006, 29, p. 1269–1274.
- Lebovitz H.E. Diabetes Rev., 1999, 7, p. 139–153.
- O’Connor P. Health Serv. Res., 2005, 6, p. 1854–1860.
- Ametov A.S., Soluyanova T.N. Medical Board, Moscow, 2011, 7–8, p. 21–24.
- Dedov I.I., Shestakova M.V. Diabetes, Moscow, 2003, p.
- Heerebek L. van, Paulus W.J. European J. of Heart Failure, 2009, 11(1), p. 3–5.
- Aleksandrov A.A., Kukharenko S.S. Yaadrihinskaya M.N. Diabetes, Moscow, 2010, 4, p. 30–37.
- Holman R., Farmer A.J., Davies M.J., Levy J.C., Darbyshire J.L., Keenan J.F., Paul S.K.; 4-T Study Group. N. Engl. J. Med., 2009, Oct. 29, 361(18), p. 1736–1747.
- Alyavi L., Grachev A. C., Musinov S.Yu., Masri M.A. Hemodynamics, remodeling and diastolic function of the heart: a Guide for masters-cardiologists, physicians functional diagnostics, therapists, Tashkent: Typography 1-TashGosMI, 2004.
- Muharlyamova M. Clinical ultrasound diagnosis: a guide for physicians: in 2 volumes, Vol. 2, Moscow, 1987, p. 296.
- Duckworth W., Abraira C., Moritz T. et al. Engl. G. Med., 2009, 360(2), p. 129–139.
- Miller R., Fincke G., Lafrance J.P. et al. Hypoglycaemia and risk of myocardial infarction in US veterans with diabetes, Presented at: European Association for the Study of Diabetes (EASD) Annual Meeting, Vienna, Austria, October 1, 2009.
- Bragd J., Adamson U., Backlund L.B. et al. Diabetes Metab., 2008, Dec., 34(6), 1, p. 612–6.