At patients diabetes 2 types noted the high frequency of bezbolevy ischemia of a myocardium (17,4 %), atypical symptoms of coronary heart disease (59,4 %), chronic warm insufficiency (60,9 %) and early development of coronary heart disease (63,8 %). Risk factors of development of coronary heart disease at patients with diabetes 2 types are the long course of diabetes, an arterial hypertension, a heavy decompensation of a carbohydrate exchange, violation of the lipidic exchange, the raised level of uric acid.
Diabetes mellitus (DM) is one of the most widespread endocrine diseases. The forecast of a current of DM, life expectancy of patients are defined by development and progressing of vascular complications: arterial hypertension (AH), nephropathy, coronary heart disease (CHD), cerebral atherosclerosis [1, 2]. At DM 2 type the risk of development of ishemia heart disease (IHD) increases by 2–4 times in comparison with population without DM. Cardiovascular diseases (CVD-SSZ) serve as a cause of death at 50–60 % of all patients suffering from DM [1]. High frequency of IHD is caused by that DM 2 types and are one of the most important risk factors of atherosclerosis as often combined with other risk factors (AH, a dyslipidemia, obesity), strengthening their adverse action [2–6].
Despite the sufficient volume of data on risk factors of development of IHD in DM 2 types, studying of clinical features of a current, risk factors of development and coronary heart disease progressing at diabetes 2 types is important problem for [3, 4] researchers.
Thus, a research objective of this work: investigation of clinical features of a current and of clinical and biochemical risk factors which are taking part in development and progressing of IHD in 2 type DM.
Materials and methods
118 patients with NIDDM which were divided for 2 groups: the first group included 69 patients with IHD, second group — 49 patients without IHD. Groups were comparable on a sex, age: 28 men (middle age of 54,4±3,3 years) and 41 women (middle age of 53,0±4,9 years) in the first group and in second — 15 men (middle age of 52,6±4,03 years) and 34 women (middle age of 51,9±4,4 years). Criteria of inclusion in research: patients aged from 45 till 60 years with IHD or without IHD. Criteria of an exception of research: the age of the patient till 45 years also is more than 60 years; existence in patients of chronic kidney insufficiency, accompanying chronic diseases, a purulent — necrotic complications. Verification of the diagnosis carried out according to criteria of Committee of WHO experts on MD (1999). For definition of the IBS form used the WHO classification (MKB — 10. T.1. P.1. С. 487): 120. Peroral sulforea and biguanides were used for treatment of 64 patients. Insulin therapy used for 54 patients (45,8 %). The average dose of insulin — 28,7±11,5 PIECES/days.
Clinical and biochemical investigation: profile of a glycemia, HbA1c, cholesterol, low density lipoproteides (LPNP), high density lipoproteides (LPVP), triglycerides (TG)), a daily proteinuria, microalbuminuriya, calculation of body weight (BWI), an index a waist circle to a circle of hips (OT/OB). All laboratory indicators were determined by the standard techniques [7, 8]. For confirmation or first time revealing of IHD was used Holterov monitoring of an electrocardiogram using «Markett HELLIGE» with computer processing of results by means of Mars 8000 system and a tredmilmetry on «HELLIGE CardioSoft V3.0». For an assessment of vegetative changes a standard autonomous electrocardiography (electrocardiograms) tests were used: test with deep operated breath (respiratory test), Valsalva's test.
Statistical analysis of obtained data is carried using computer with application of packages of the applied programs «Biostats» and «Statistica 6.0». All data are presented as arithmetic averages and their standard deviation (М±SD). Reliability of distinctions was estimated by means of t-criterion of Student at normal distribution of a sign and in other cases — using of Mann's nonparametric method Whitney. For the analysis of qualitative signs were used Fischer's exact criterion and χ2. Reliability of coefficients of distinctions accepted at value р < 0,05. For establishment of interrelation of signs carried out the correlation analysis according to Pearson (at normal distribution of a sign) or across Spirmen (at distribution of a sign, excellent from normal).
Results
Among patients with NIDDM the IHD following forms were revealed: tension stenocardia — 60,9 % (42 patients); previous infarct of myocardium — 60,9 % (42 patients); ischemia of a myocardium — 17,4 % (12 patients). At 13 (18,9 %) (9 men, middle age of 53,6±3,9 years; 4 women, middle age of 54,8±2,9 years) IHD was verified on average for 3,5±1,6 earlier, than diabetes was distinguished. From them at 6 (46,1 %) IHD was diagnosed aged from 45 till 50 years and at 7 (53,9 %) patients are more over 50 years. In 3 (4,3 %) (2 men, average age — 57,5±2,1 years; 1 woman — age of 46 years) cases of NIDDM and IBS were diagnosed at the same time. At 53 (76,8 %) patients (15 men, middle age of 54,2±2,8 years; 33 women, middle age of 52,8±5,1 years) NIDDM was diagnosed for 7,3±3,5 years before IHD development. From them in 9 (17 %) patients IHD was revealed aged till 45 years, in 27 (50,9 %) — from 45 to 50 years and in 17 (32,1 %) patients are diagnosed over age as 50 years.
In 12 (17,4 %) patients (4 men, middle age of 56,7±2,6 years; 8 women, middle age of 52,6±4,8 years) painless form of ischemia of myocardium is revealed. From them at 7 patients have diagnosis as stenocardia of tension. Duration of a disease of NIDDM at patients with painless form ischemia of myocardium proceedes 5,5±4,9 years.
Among patients with NIDDN and IHD at 42 (60,9 %) age 53,7±5,5 years had previously IM: 18 men (middle age 54,0±3,2 years) and 24 women (middle age 52,5±5,1 years). Duration of NIDDM in patients with myocardial infarction preceding it — 10,2±7,4 years.
In patients with NIDDM+IHD 23 persons (33,3 %, 10 men and 13 women) 3 persons had the expressed heartaches developed after physical exercises. 41 patients (59,4 %) in were found atypical symptoms, from them 27 people (9 men and 18 women) have aching heartaches accompanied by fatigue and weakness and 14 people (7 men and 7 women) have heartaches not connected with physical activity.
Results of Holterov monitoring: in 5 patients painless ischemia of a myocardium was revealed, and in 7 patients — stenocardia of tension noted bezbolevy episodes of ischemia of a myocardium. In 22 patients with atypical symptoms a shift of a segment of ST according ischemic type was registered.
The cardiovascular form of the diabetic autonomous neiropathy (DAN) was revealed in patients of 1 group with existence of atypical symptoms of IHD in 92,7 % cases, from them — among patients with painless ischemia of a myocardium in 91,7 % cases, among patients with typical with typical pain behind a breast — in 82,6 % cases (Fig. 1). Respiratory coefficient and values Valsalva's coefficient had no reliable differences depending on a clinical current of IHD (6,0±3,9 and 1,00±0,09; 5,0±4,2 and 1,02±0,09; 6,1±5,6 and 1,03±0,09 respectively, p > 0,05).
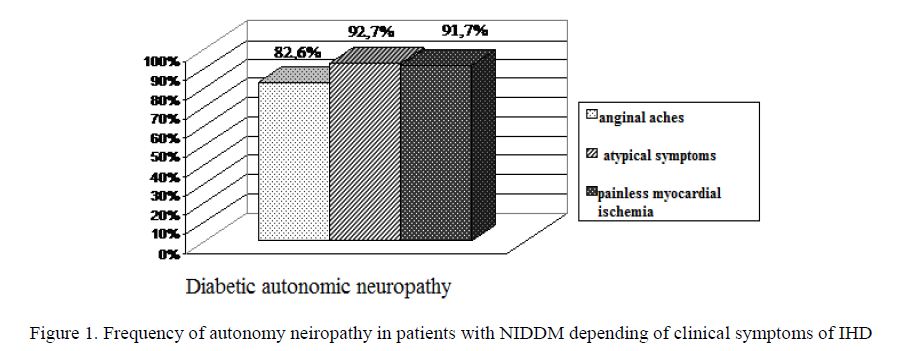
Figure 1. Frequency of autonomy neiropathy in patients with NIDDM depending of clinical symptoms of IHD
In patients with NIDDM + IM Diabetic Autonomy Neuropathy (DAN) was found in 92,9 %. In patients with IM and without as without it the average values of coefficient of Valsalv’a and test with breath authentically didn't differ (1,02±0,09 and 5,6±4,3; 1,02±0,09 and 5,5±4,5 respectively, p > 0,05).
As result of clinical investigation of 20 patients (9 men and 11 women) with NIDDM with IHD is revealed the chronic heart insufficiency (CHI) of the I functional class (FC) according classification of the New York association of the heart (NYHA), the II FC — in 18 persons (6 men and 12 women) and III FC — in 4 patients (2 men and 2 women). Average age of sick SD 2 types with CHI FC I made 54,8±4,4 years, with the II FC — 54,0±3,7 years, with the III FC — 57,0±2,7 years. The interrelation of duration of a current of NIDDM, AG, IHD and FC CHI are investigated. Thus, patients with the III FC CHI had higher duration of IHD. So at the I FC IHD duration of IHD was prolonged 3,9±2,5 years, in the II FC — 6,4±3,2 years, and in patients with III FC HSN — 9,0±7,1 years (р <0,05).
One of research problems was investigation of clinical and biochemical risk factors which are taking part in development and progressing of IBS at sick SD 2 types. By results of this research Duration of NIDDM prevailed at patients with IHD comparatively with patients without it (8,7±5,9 and 6,5±5,2 years respectively, р < 0,05). Women with IHD had duration of NIDDM authentically above, than at patients is a male which made 10,3±5,7 and 7,5±5,3 years respectively, (р < 0,01). Duration NIDDM at women with IHD authentically prevailed in comparison with patients without it (10,2±6,4 and 5,8±5,1 years respectively, р < 0,001).
Prevalence of AG at patients with NIDDM made 96,6 %. AG duration in patients with NIDDM and IHD made 10,3±5,7 years and in patients with NIDDM without IHD 7,5±5,3 of years (р < 0,05). AG duration at women with NIDDM and IHD authentically prevailed comparatively with women without IBS which made 11,6±6,2 and 6,9±5,6 years, respectively (р < 0,01). Among patients with NIDDM and IHD according to MOAG (1999) WHO classification 2nd degree of AG is revealed in 28,9 % of patients, the 3rd degree of AG in 71,1 % cases. In patients without IBS 2nd degree of AG is established in 30,6 %, the 3rd degree of 61,2 % cases and at 4 (8,2 %) patients weren't noted arterial pressure (AP) increase ((c2 = 6,068, р = 0,048). Patients with IHD had systolic arterial pressure (SAP) and diastolic arterial pressure (DAP) indicators authentically above than in patients without IHD.
Tobacco smoking frequency in patients with NIDDM made 46,6 % and in patients with NIDDM and IHD (55,1 %) in comparison with in patients with NIDDM and without IBS (34,7 %) (χ2 = 3,998, р = 0,046). Among patients with IHD the percent of smoking men made 96,4 %, and among patients without IHD — 86,7 % (χ2 = 0,324; р = 0,569). Female patients with NIDDM with IBS smoked in 26,8 % cases, women with NIDDM without IHD in 11,8 % cases (χ2 = 1,779, р = 0,182).
High prevalence of IBS and other diseases of cardiovascular system at SD is defined by also such factors as a hyperglycemia, insulin resistance and giperinsulinemya, obesity, low physical activity, a dislipidemya.
The Body Weight Index (BWI) was raised in both groups. At patients of SD 2 types with IHDS BWI on average made 33,1±5,5 kg/sq.m, in patients without IHD — 30,8±6,8 kg/sq.m (р > 0,05). Irrespective of existence or abscence of IHD, a high values of an index «a waist circle to a circle of hips (OT/OB)» are revealed. Among men with NIDDM and IHD and without IHD the abdominal type of obesity is established 82,1 % and 73,3 % cases correspondingly (χ2 = 0,080, р = 0,777), among women in 92,7 % and 88,2 % cases respectively (χ2 = 0,068, р = 0,794).
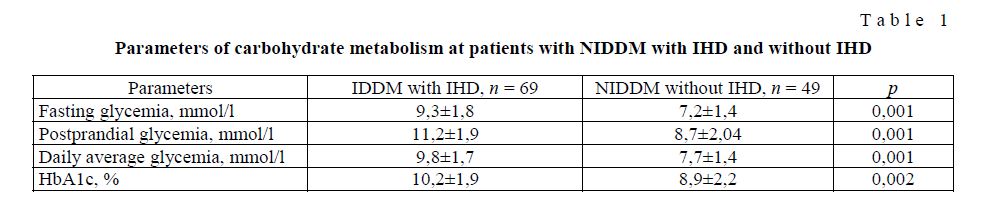
When studying indicators of a carbohydrate exchange at sick SD 2 types with IBS in comparison with patients of SD 2 types without IBS are revealed. A higher levels of morning glycemia (р<0,001), a postprandial glycemia (р < 0,001), an average daily glycemia (р < 0,001) and HbA1c (р < 0,01) were revealed in patients with NIDDM +IHD omparatively with NIDDM only (Table 1).
T a b l e 1
Parameters of carbohydrate metabolism at patients with NIDDM with IHD and without IHD
Lipid metabolism disorders. According to criteria of European Diabetes Policy Group (1998–1999) patients with NIDDM and IHD the hypercholesterolemia (>4,8 mmol/l) is revealed in 88,4 %, in patients without IBS in 73,5 % (χ2 = 3,408, р = 0,065), a hypertriglyceridemia (>1,7 mmol/l) 82,6 % and 57,1 % cases respectively (χ2 = 8,003, р = 0,005). The LPNP high level (>3,0 mmol/l) at patients of 1 group was defined at 72,5 %, in 2nd group at 51,0 % of patients (χ2 = 4,800, р = 0,028). Low concentration of LPVP (>1,2 mmol/l) was observed at 68,1 % patients with NIDDM with IBS and at 38,7 % of patients without IBS (χ2 = 11,584, р = 0,001). The Atherogenic Coefficient (AC) was higher at patients with NIDDM and IHD (82,6 %) in comparisons with patients without IBS (63,3 %) (χ2 = 4,680, р = 0,031) (Fig. 2).
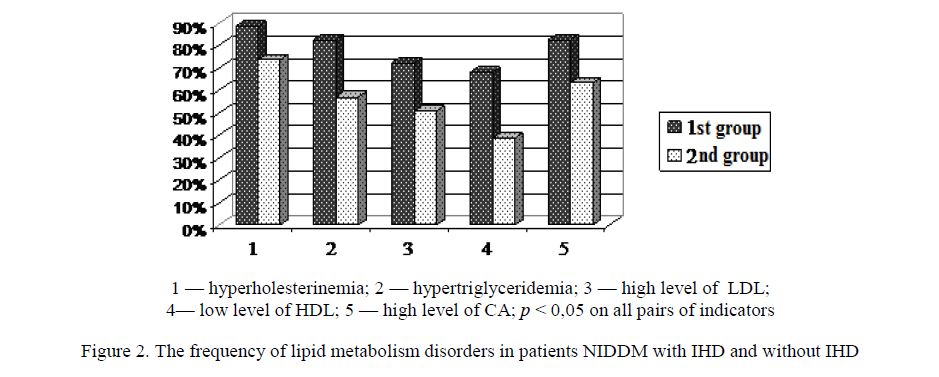
Figure 2. The frequency of lipid metabolism disorders in patients NIDDM with IHD and without IHD
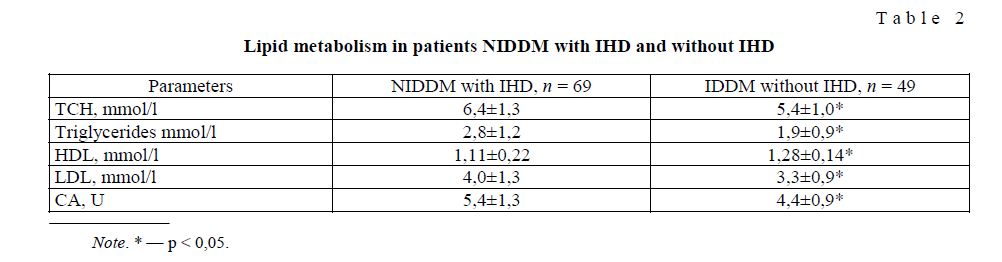
Apparently (Table 2), patients with IHD had on average values of OHS, TG, LPVP authentically higher than at patients without IHD. Statistically significant decrease concentration of LPVP showed noted at patients with NIDDM and IHD in comparison with patients without IBS (р < 0,001). Authentically the KA high levels are revealed in patients with NIDDM.
Lipid metabolism in patients NIDDM with IHD and without IHD
T a b l e 2
Miroalbuminuria is revealed in 56,5 % number of patients with NIDDM and IHD and in 40,8 % patients without IBS (χ2 = 2,234, р = 0,135). The proteinuria was found in 28,9 % of patients of 1 group and in 24,5 % of (χ2 = 0,110, р = 0,741).
The content of uric acid in both groups without changes. However, in patients with NIDDM and IHD had an average value of uric acid authentically above than at patients without IBS (303,5±71,5 and 264,8±51,3 mmol/l respectively, р < 0,05).
By correlation analysis of patients with NIDDM and IHD it was revealed significant interrelations between morning glycemia and duration of NIDDM (r = 0,36, p < 0,05), the TG level (r = 0,47, p < 0,05), LPVP (r = –0,41, p < 0,05). Similar data are obtained for postprandial glycemia: interrelation with values of LPNP (r = 0,21, p < 0,05), uric acid (r = 0,31, p < 0,05) and diastolic arterial pressure (r = 0,20, p < 0,05) also was revealed. The HbAc1 level didn't correlate with NIDDM duration and with level of TG and LPNP, LPVP, uric acid, meanwhile was however connected with the OHS level of serum of blood (r = 0,24, p < 0,05).
42 patients with NIDDM (60,9 %) patients have earlier a myocardial infarction. patients with NIDDM with IHD and IM in the anamnesis and without IM only reliable distinction on NIDDM duration is noted, but not revealed statistically significant difference on BWI, AG duration, to the GARDEN and DAD levels, indicators of a carbohydrate and lipid changes, values of uric acid, a daily proteinuria.
Discussion
Frequency of combination of NIDDM and IHD can reach 45–55 %, and IHD developed early [5, 9–12]. Our results confirmed a high frequency of IHD in patients with NIDDM as 58,5 %; more often among persons till 50 years (63,8 %) testify to the high frequency of IHD.
According to some authors at sick SD 2 types Existence of an autonomous neiropathy with alteration of afferent nerves of heart can be one of cause developing of painless ishemia of a myocardium and atypical symptoms of IHD which increase risk development of sudden death [2, 7, 10, 13]. It is necessary treat of all symptoms of ischemia of a myocardium not only of typical attacks of stenocardia.
NIDDM consider as one of major factors of risk of heart function insufficiency. At patients with NIDDM types with IHD in 60,9 % cases there are a chronic heart insufficiency which depended of NIDDM duration. These data are coordinated with Framingemky's results, results of the Russian epidemiological research EPOHA-HHI as with American national register NHANES.
High frequency of cardiovascular diseases in patients with NIDDM is caused by various risk factors. In diabetes the risk of development of IHD may be determinaed by obesity, smoking, AG, a dislipidemiya, and also with a hyperglycemia, an insulin resistance and by hyperinsulinemia. Our results showed that in patients with NIDDM+IHD duration of diabetes and AG of the GARDEN and DAD level authentically more high and fact of smoking is established more often comparatively with patients without IBS. The Body Weight Index as a giperinsulinemia indicator, was increased as high values of index a waist circle to a circle of hips (OT/OB) as in patients with NIDDM+IHD as in NIDDM without IHD. It is a not direct confirmation of importance role of smoking and AG as of abdominal obesity in development of macrovascular complications in NIDDM. More high morning and postprandial glycemia and HbA were revealed in patients with NIDDM+IHD as more high frequency of hyper triglycerinemia more high level of LPLD and KA level, the low concentration of LPHD omparatively with patients with NIDDM only.
Researches UKPDS (1998), Honolulu Heart Study (1999), DECODE (The Diabetes Epidemiology: Collaborative Analysis of Diagnostic Criteria in Europe) (1999) established reliable decrease of the frequency of macrovascular complications among patients with lower glycemia level and also adverse predictive value of a postprandial hyperglycemia in development of cardiovascular complications [14].
Thus, results of this research confirm important role of disorders of the glucose and lipid metabolism as risk factors of atherogenesis.
Today more often the great significance is attached to influence of factors as microalbuminuria, proteinuria and of uric acid as risk factors for developing of cardiovascular diseases.
Among patients with NIDDM+IHD frequency of a microalbuminuria made 56,5 % that will be coordinated with results of D.R.Meeking et al. (1999) [15]. Patients had authentically more high aised level of uric acid comparatively with patients with NIDDM only. Microalbuminuria is a marker developing of atherosclerosis [9] and the raised content of uric acid can promote damage endothelium of arteries and create predisposition to fixation of cholesterol, to activate adhesion and aggregation of platelets [16].
Conclusions
- In patients with NIDDM are revealed the high frequency of painless form of ischemia of a myocardium (17,4 %), atypical symptoms (59,4 %) of IHD, chronic heart function insufficiency (60,9 %) and in 63,8 % early development of IHD (till 50 years).
- In patients with NIDDM+IHD is revealed longer current of NIDDM and of AG, decompensation glucose metabolism and marked disorders of a lipid metabolism as high frequency of the hypertriglyceridemiya, high LPNP level, and low level of LPVP, authentically high level systolic and diastolic blood pressure as of uric acid concentration comparatively with patients without
References
- Аmetov A.S., Solovieva O.L. Russian Medical Journal, 2011, 27, p. 12–14.
- Аmетоv А.S., Demidova T.Y., Kosych S.A. Problems of Endocrinology, Moscow, 2005, 4, p. 3–6.
- Аmетоv А.S. Diabetes mellitus 2 type. Problems and decision, GEOTAR-Меdia, 2013, 1032
- Аrakelianz А.А., Gorohova S.G. Russian Journal of cardiology, 2004, 1, p. 80–86.
- Balabolkin M.I., Klebanova E.M., Kreminska V.M. Treatment of diabetes and its complications, Moscow: Medicine, 2005, 512
- Birukova E.V. Russian Medical Journal, 2010, 14, p. 6–9.
- Gurevich M.A. Russian Medical Journal, 2005, 6, p. 49–52.
- Dolgov V.V. Clinical and laboratory diagnostic (national issue), GEOTAR-Меdia, 2012, 1, 928
- Кuimov A.D. Miocardial infarct in women, Novosibirsk: Nauka, 2006, 132
- Orlov V.A., Urusbieva D.M. Russian Journal of cardiology, 2001, 5, p. 89–98.
- Chasova T.E., Kathuria Y.B. Medical service, 2001, 5, p. 28–32.
- Jermendy G., Davidovith Z., Khoor S. Diabetes Care, 1994, 17, p. 1231–1232.
- Johnson R., Kivlighn S., Kim Y.G. et al. Am. J. Kidney Dis., 1999, 33, p. 225–234.
- UK Prospective Diabetes Study (UKPDS) Group. Lancet, 1998, 352, p. 837–853.
- Krempf M., Steg P., Bhatt D. et al. Diabetologia, 2006, 49, 1, p. 231–232.
- Meeking D.R. et al. Diabet. Med., 1999, 16, p. 841–847.