Studied 55 samples of the blood of patients with chronic myeloid leukemia. Investigated two options translocation t (9; 22). As a method used by polymerase chain reaction in the real-time mode. In 52,73% of the objects of study found Philadelphia chromosome. Studied the transcript of the gene.
Chronic myeloid leukemia (CML) is the most frequently diagnosed case of the all chronic myeloproliferative diseases, which are affecting pluripotent stem cells of precursor myeloid, erythroid, B-lymphoid cells and megakaryocytes, also this is one of the common types of leukemia, occurring in 20 % of all cases of leukemia. Nearly a half of all patients usually discover the disease in the period of their higher professional and social activity, when they are between 30 to 50 years old [1, 2].
The characteristic feature of the disease is the fact of the detection of Philadelphia chromosome (Phchromosome), or a specific reciprocal translocation, which is occurring between the chromosomes 9 and 22: t (9; 22) (q34; q11). It is well-known that those translocation represents by itself simply the result of the merger of the two genes, BCR-ABL in Ph-chromosome and ABL-BCR 9q. BCR-ABL encodes the formation process of protein with a higher level of tyrosine kinase activity, which is considered as the central mechanisms in the chronic phase of CML. This kind of karyotype change was found in 95 % of CML cases, so, that’s why this (9; 22) may be considered as especial sign of CML. Furthermore, Ph-chromosome was found in 25 % of patient cases as the acute lymphoblastic leukemia (ALL) and in 2 % of patient cases as the acute myeloid leukemia (AML) [3, 4]. On this moment the most effective Ph-detection method is the polymerase chain reaction (PCR) [5, 6].
The main purpose of this work is the detecting of the translocation t (9; 22) by the method of real-time PCR («Real-time PCR») in all patient cases, which have chronic myeloid leukemia [7].
Materials and methods
As a material for the research we had take the samples of peripheral blood of these patients, who were on a survey in the hematological department of the regional clinical hospital and also in the children's cancer and blood diseases center of Karaganda. Patients’ age ranged from 1 to 60 years old. During the all molecular genetic manipulations we used the reagents of firm «Amplisens».
After the taking RNA from the blood, for the obtaining of cDNA, we were gaining the reverse transcription reaction by the «Tertsik» device. The amplification and the detection of PCR products for a long time were holded in our device «DT-322» (manufactured by «DNA-technology»).
All manipulations with all clinical specimens (RNA picking out, holding the reaction of reverse transcription for the obtaining of cDNA, PCR and the detection of all amplification products) were carried out in the strict accordence with all instructions, which had been attached to all reagents complex and the requirements for PCR laboratories [8].
Results and discussion
For obtaining of the desired fragment we isolated RNA from the peripheral blood cells. The method of allocation of mRNA BCR-ABL from single clinical material is based on the extraction of total RNA. Then the samples were subjected to the reaction of reverse transcription with the using of the enzyme revertazy. Polymerase chain reaction and the detection of the amplification products were carried out by us in real time regime with the using of two mixtures of oligonucleotides: the amplification plot of mRNA chimeric gene M-bcr-abl (p-210), which corresponds to the relevant section of cross-linking genes bcr and abl (b2a2 and b3a2) and a fragment of mRNA splicing gene N-abl, (which is recommended by the working group of «Europe Against Cancer», EAU) as an endogenous internal control (EIC) and the gene-normalizer.
6 variants of translocation t (9;22) with formation of philadelphia chromosome is described [3]. They are represented on the figure 1. Two from them (b2a2 and b3a2) was studied in this research.
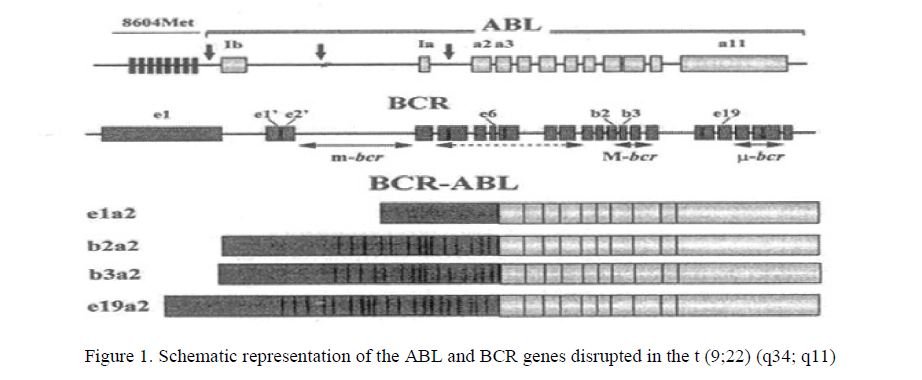
Figure 1. Schematic representation of the ABL and BCR genes disrupted in the t (9;22) (q34; q11)
The presence of the endogenous internal control allows to control the main stages of analysis, including the fence, transporting, storing samples, RNA, carrying out the reaction of reverse transcription of RNA and amplification of cDNA.
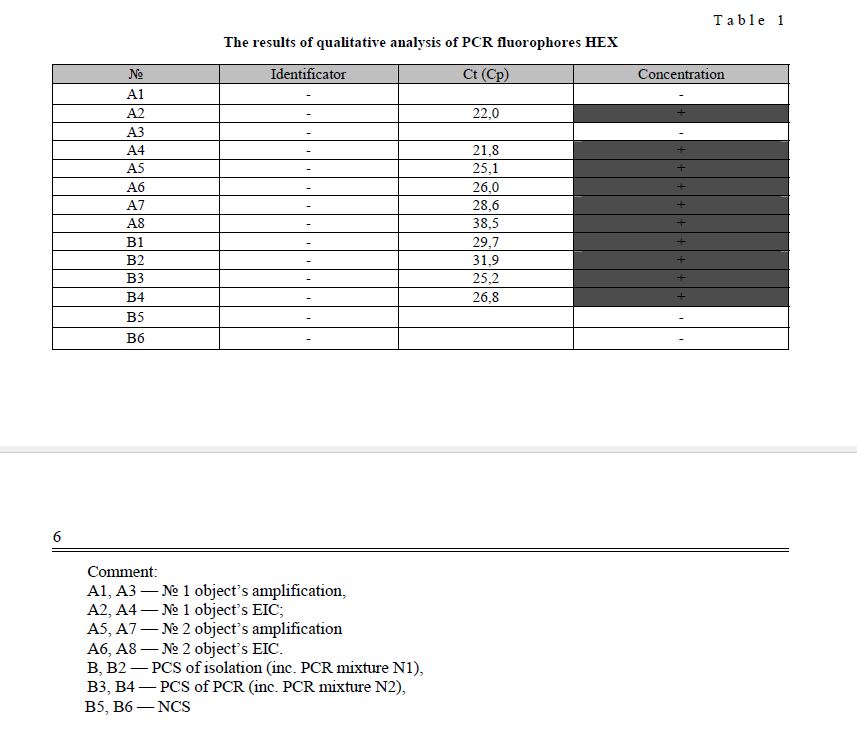
During the process of each work stage, we used the positive and the negative control samples (PCS and NCS). For the control in time of the various analysis stages (picking out of RNA and polymerase chain reaction) there were used two types of positive controls: PCS allocation (including the mixture N allocation in the PCR), PCS PCR (including the mixture N allocation in the PCR). The result of amplification of cDNA bcr-abl and abl recordes with the using of HEX fluorescence. The specificity of the reaction proposes the holding of all reactions in two replications. The results of 2 from all 55 tests are showed in Table 1.
v
T a b l e 1
During the 13 months of 2008 and 2009 we had 55 tests of peripheral blood of patients, who were hospitalized to the hematology department of the regional clinical hospital of Karaganda city and to the Regional Cancer and Blood Diseases Children's Center ambulatory with the possible diagnosis — the chronic myeloid leukemia. During the research of Philadelphia chromosome, we were taking into consideration the different age groups. Due to the work purpose was the determining of the unfavorable environmental factors on the formation of the translocation t (9; 22), we pointed among other factors the place of patient’s residence.
All inspection results are presented in Table 2.
The patients’ data
T a b l e 2
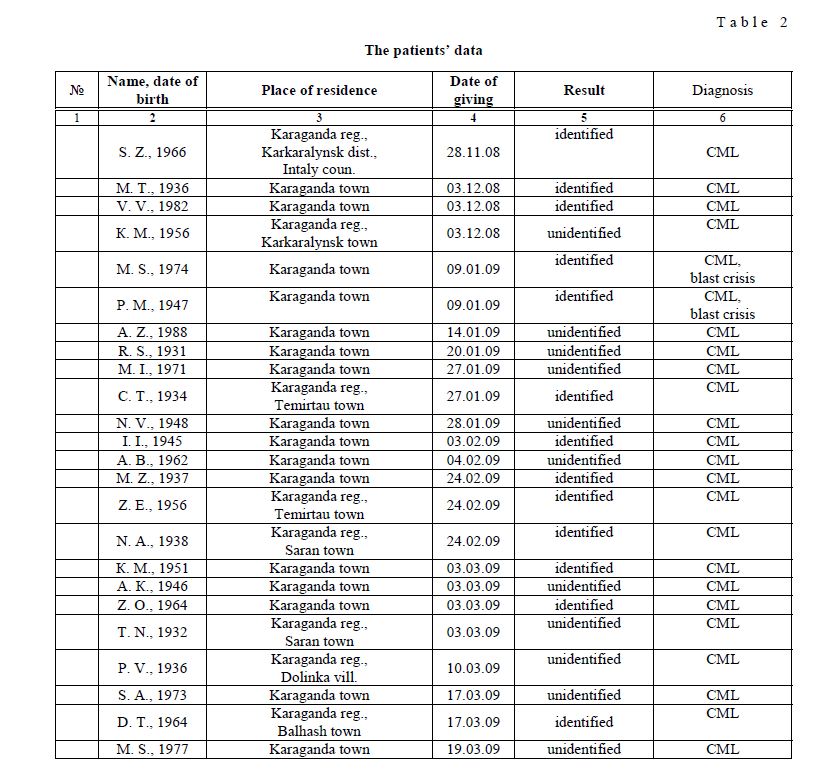
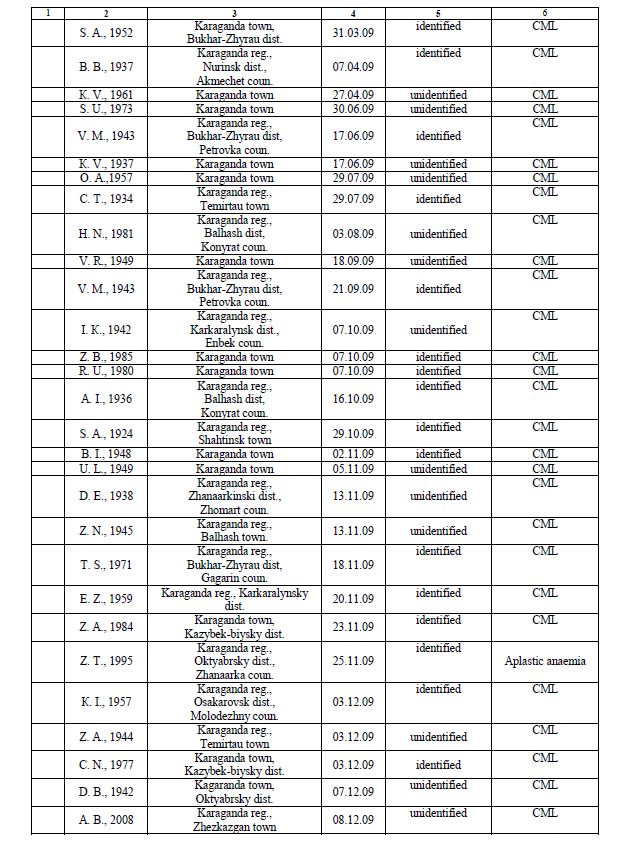

As we may see from the table, nearly in 29 of 55 patients’ cases, there is the diagnosis of Phchromosome. In percentage terms, detected disease takes 52,73 %. At the same time, according to published scientific data, the translocation t (9; 22) usually occurs in 95 % of all cases of CML [3]. It is well-known that the cause of chronic myeloid leukemia may be other variants of this translocation and other chromosomal rearrangements, which are not considered by us in the present work.
Summary results of our studies are represented on the figure 2.
Figure 2. Detection of translocation t (9; 22) 1 — samples without Ph-chromosome; 2 — patients with translocation t (9; 22)
This figure is demonstrated that in 52,73 % of studied samples translocation (9; 22) was detected. Consequently in these cases philadelphia chromosome from the patients with chronic myeloid leukemia was find.
Further researches suggest the scientific review of various forms of leukemia by the other translocation cause malignant tumors method.
Bibliography
- Volkova A. Glivec during the chronic myeloid leukemia-achievements, failures, problems // Hematology and Transfusiology. — 2004. — Vol. 49(2). — P. 35–41.
- Bogdanov K.V., Frolova O.I., Marinec O.V. et al. The clinical significance of the variants of the chromosomal translocation t (9; 22) in patients’ cases with the chronic myeloid leukemia // Hematology and — 2003. — Vol. 48(3). — P. 9–13.
- Melo V. The Diversity of BCR-ABL Fusion Proteins and their relationship to leukemia phenotype // Blood. — 1996. — Vol. 88(7).
- Daley G.Q., Etten R.A., Baltimore D. Induction of Chronic Myelogenous Leukemia in Mice by the P210 Bcr/Abl Gene of the Philadelphia Chromosome // Science. — 1990. — Vol. 247. — P. 824–830.
- Tajeddine N., Millard I., Gailly P. and Gala J.L. Real-time RT-PCR quantification of PRAME gene expression for monitoring minimal residual disease in acute myeloblastic leukemia // Chem. Lab. Med. — 2006. — Vol. 44(5). — P. 548–556.
- Imyanitov E.N., Komochkov I.V., Lyschev A.A., Togo A.V. The molecular and clinical oncology: the point of contact // Onc. — 1993. — Vol. 5. — P. 3–8.
- Radich J.P., Gooley T., Bryant E. et al. The Significance of Bcr-Abl Molecular Detection in Chronic Myeloid Leukemia Patients «Late» 18 Months or More After Transplantation // Blood. — 2001. — Vol. 98(6). — P. 1701–1707.
- Burmeister T., Maurer J., Aivado M. et al. Quality assurance in RT-PCR-based BCR/ABL diagnostic — results of an interlaboratory test and a standartization approach // Leukemia. — 2000. — № 10. — P. 1850–1856.