In this article, we described a clinical case that confirms that splenecto my as a method of treatment of complications of idiopathic myelofibrosis has sufficient efficacy, especially in portal hypertension, compression syndrome and hemolytic anemia, which can significantly improve the quality of life of patients, although it does not prolong its duration significantly. In this patient, surgical treatment passed without complications, led to an improvement in overall well-being.
Idiopathic myelofibrosis (IMF) is a rare disease, the number of newly diagnosed patients who are 1: 100 000 a year. Synonyms of the disease: osteomyelophybrosis, primary myelofibrosis, subleukemicmyelosis.
Pathogenetically, IMP is a bone marrow disease in which the proliferation of descendants of transformed hematopoietic stem cells leads to fibrosis and the replacement of the active bone marrow with collagen fibers. Treatment of IMP is a complex and urgent problem. One of the complications of IMP is hepatosplenomegaly. If there is a risk of rupture of the spleen and intra-abdominal hemorrhage, surgical interventions are necessary.
Surgical treatment (splenectomy, correction of manifestations of portal hypertension) is an additional method aimed at correcting complications of the disease. Indication for splenectomy is a giant splenomegaly with a syndrome of hypersplenism, compression of internal organs and vessels, insufficient effect of drug therapy, cachexia. In most cases splenectomy brings improvement in the form of reducing symptoms (pain relief, bloating, weight loss), which improves the quality of life of the patient. At the same time, enlarged spleen, portal hypertension, violation of hemostasis cause significant difficulties in the operation in 30-50% of patients lead to postoperative complications, and 5-10% to lethality. The overall survival of patients with IMP after splenectomy is about 2 years and does not affect the overall life expectancy of patients. Idiopathic myelofibrosis in the vast majority of cases is diagnosed at the age of 50-70 years.
case from practice:In this connection, the case of splenectomy in the patient is 66 years old.
Patient D., 66 years old, was urgently hospitalized in GKB No. 7 hematology department with the diagnosis: Idiopathic myelofibrosis, terminal stage. Tumor intoxication. Secondary immunodeficiency state. Chronic bronchitis, exacerbation. Respiratory failure 0. Cirrhosis of the liver, secondary genesis. Portal hypertension. Hepatosplenomegaly. Osteo-ascitic syndrome. Ascite of the 1st degree. Concomitant diagnosis: Arterial hypertension 2 degrees, risk 3. Chronic heart failure 1. Functional class 3. complaints on admission: an increase in temperature to 38-39 ° C, general weakness, dyspnoea with physical exertion, malaise, bone pain, fatigue.
Anamnesis of the disease. Consists of "D" accounting from a hematologist since 1995. Clinical diagnosis is established on the basis of a tumor-intoxication syndrome, hemograms (normochromic anemia, leukocytosis, thrombocytosis, accelerated ESR), myeloproliferative syndrome (hepatosplenomegaly), cytological bone marrow examination, bone marrow histology (trepanobiopsy). Monochemotherapy with hydra was conducted, with accompanying therapy. There were repeated courses of chemotherapy: cytosar "small" doses, with accompanying therapy, blood transfusion.
This deterioration of the condition was noted during the week: the phenomenon of tumor-intoxication syndrome. 07.08.16. The patient was taken by ambulance brigade in State Clinical Hospital №7.
The general analysis of a blood 07.08.16: erythrocytes-3.1 * 1012 / l. leukocytes-33.3 * 109 / l. Нв 93 g / l, platelets-248 * 109 / l.
Biochemical analysis of blood 07.08.16: total bilirubin-15.3 mmol / l. urea-8.4 mmol / l. Creatinine of blood-65,2mol / l.
Ultrasound examination of the abdominal cavity organs from 30.05.16: Severe splenomegaly. Hepatomegalia. Signs of diffuse changes in the liver parenchyma, spleen. Signs of portal hypertension.
Anamnesis of life. According to the patient grew and developed according to age. Heredity is not burdened. Botkin's disease suffered as a child. Viral hepatitis, tuberculosis, skin-venereal diseases is denied. Allergic anamnesis: According to the allergy to the following medicines: Analgin, Dimedrol, Riboxin, Vitamin B1, B6. Consists on dispensary registration with the therapist with the diagnosis: Hypertension II degree, risk 2. Periodically takes antihypertensive drugs. Surgery in history: appendectomy (1995), hernioplasty (1998) for a hernia of the white line of the abdomen. Blood transfusion of blood components in August 2016 was associated with severe anemia.
objective inspection. At admission, the general condition of the patient is severe, due to the tumor-intoxication, pronounced myeloproliferative (splenomegaly) syndromes. Body hyposthenic,undernutrition. Consciousness is clear, the patient is listless, hypodynamic. Skin pale, clean. Zev is calm. Peripheral lymph nodes are not palpable. Bone-joint system: without visible pathology. In the lungs, the breath is vesicular, there is no wheezing. The respiratory rate is 16 in min. Borders of relative cardiac dullness widened to the left + 0.5 cm. Heart sounds are muffled, rhythmic. AD - 110 / 70mmHg, pulse - 80 in min. The language is wet, clean. The abdomen is enlarged in size due to pronounced splenomegaly, soft, painless. The liver protrudes from under the edge of the costal arch by 4 cm. The spleen occupies the entire left half of the abdominal cavity. The chair and diuresis are normal.
Laboratory-diagnostic studies were carried out:
The general analysis of a blood: erythrocytes - 4,0 * 1012 / l. Hв - 113 g / l. leucocytes - 39,3 * 109 / l. platelets - 321 * 109 / l. myelocytes -19%, stab-9%, segment-nuclear -46%, basophils - 4%, monocytes -2%, lymphocytes-10%, ESR -30 mm / h. Biochemical blood test: glucose -3.8 mmol / l, total protein -62.3 g / l, AlaT-4 u / l. AsaT-17.1 u / l. Blood creatinine -52 μmol / l. Urea -7.5 μmol / l, sodium -143 mmol / l, potassium -4.10 mmol / l, calcium -1.22 mmol / l. Coagulogram: TV-14,9s, AChTV -45.50s, MNO -1.55s, PTI -57.8%, PV-21.6s, fibrinogen A 3.9g / l. Microrection №705157 - negative. ELISA for HC markers: HBsAg-
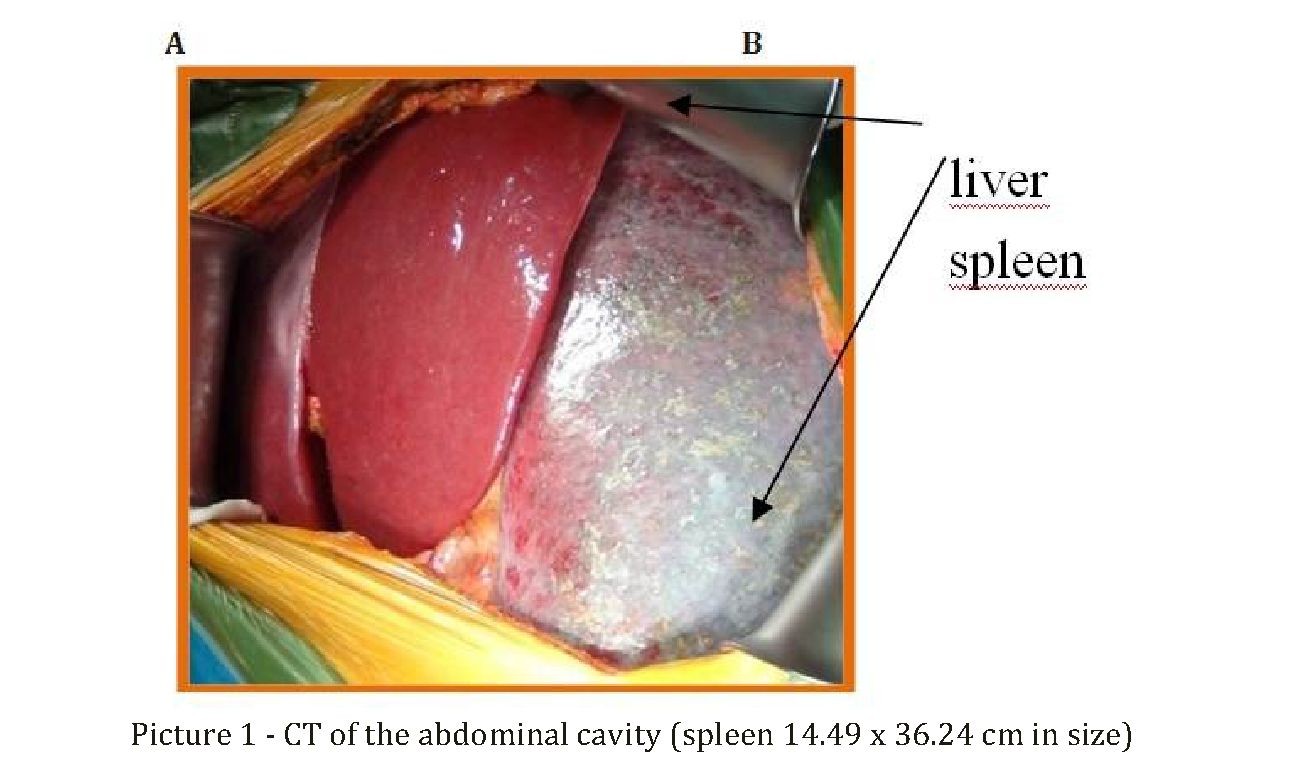
negative, Anti-HCV-negative. # 70515825. HIV antibody test: otr No. 1301036759; OAM: count-100ml, s / w, transparent, rel. Dense-1020, protein-0,099g / l. watering-1-2 sp. Radiography of the Organs of the chest - chronic bronchitis. ECG: rhythm sinus rhythm with heart rate = 90 in min. Vertical position of EOS. Ultrasound examination of the abdominal organs: hepatosplenomegaly. Diffusive changes in the parenchyma of the liver, pancreas. Signs of hemangioma in the parenchyma of the spleen. (the area of the spleen is 286.0 cm2). CT examination of the abdominal cavity and retroperitoneal space with bolus contrast: pronounced splenomegaly, with microcalcinate and fibrosis areas in the structure. Pericarditis, bilateral pleural layers. Diffusive changes in the liver and pancreatic parenchyma, with hepatomegaly, ascites. The tendency of fatty hepatosis with the phenomenon of portal hypertension. Chronic cholecystitis. Two-sided chronic pyelonephritis, with pyeloectasia with microlites. Pathological bone reconstruction in the chest-lumbar spine and pelvic bones (Figure 1). FGDS: chronic reflux-gastritis. Ultrasonic examination of pelvic organs: interstitial uterine myoma, multiple (two m / y).
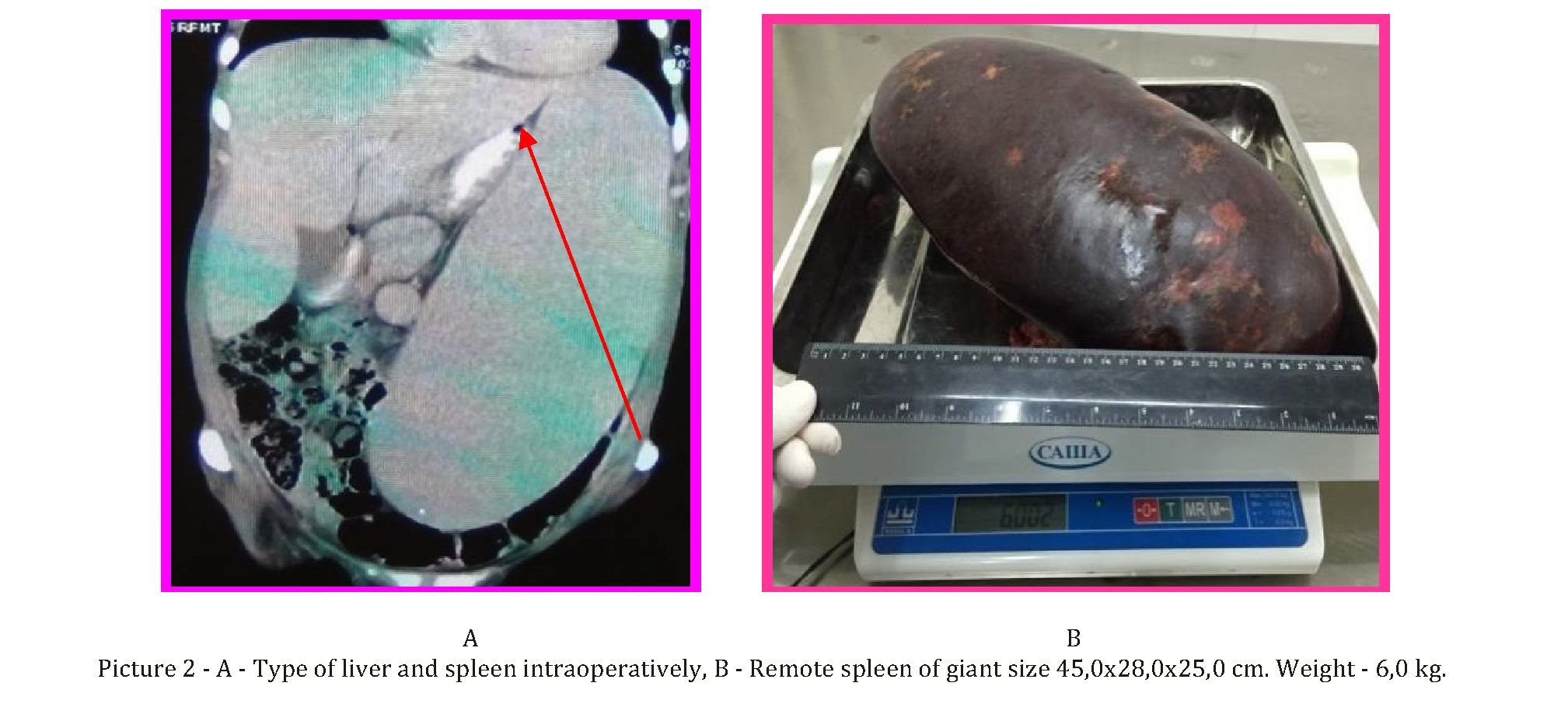
The patient was examined by a surgeon, in connection with abdominal pain on 27.09.16. The patient was transferred to the department of planned surgery splenectomy. On September 28, 2016, after preoperative preparation under endotracheal anesthesia, an upper-median laparotomy was performed. There is no effusion. At revision of organs of an abdominal cavity the liver is enlarged, usual color, dense consistence, a surface smooth. Gall bladder 6,0x3,0 cm, not stressed, wall not thickened, holedoch not widened (0.4 cm). The spleen is enlarged in size 45.0 x 28.0 x 25.0 cm, dark-burgundy in color and dense in consistency. Other organs of the abdominal cavity without features. Selezonochnaya artery and vein are enlarged in diameter. Then the spleen was mobilized with the intersection of short gastro-splenic veins and doping. The splenic artery is mobilized, clamped, crossed and doped twice. The sepulchral vein is treated with the "Hem-o-lok" clipper, crossed. Splenectomy was performed. Hemostasis is dry during the operation. Through the counter-percutaneous incisions on the left, the left sub-diaphragmatic space and the small pelvis are drained.
Postoperative diagnosis: Idiopathic myelofibrosis, terminal stage. Tumor intoxication. Hepatosplenomegaly.
The postoperative period proceeded without complications. Drainage pipes are removed on the third day. 07.10.2016 skin seams were removed, the wound healed by primary tension. The patient is in a satisfactory condition discharged to outpatient treatment at the place of residence.
10/17/2016, the patient's control examination: the condition is satisfactory, recommendations on the observation and treatment of the underlying disease in the hematologist are given.
Conclusion. Splenectomy as a treatment for complications of idiopathic myelofibrosis has not lost its positive values, have sufficient efficacy, especially in portal hypertension, compression syndrome and hemolytic anemia, can significantly improve the quality of life of patients, although not significantly prolongs its duration. In this patient surgery went without complications, led to an improvement in general well-being.
REFERENCES
- Vannuchi A., Gudlielmelti P., Tefferi A.et al. Progress in understanding myeloproliferative neoplasms // Cancer J Clin. – 2009. - №59. – Р. 171–191.
- Tefferi A., Thiele J, Vardiman J.W. The 2008 World Health Organization classification system for myeloproliferative neoplasms: order out chaos // Blood. – 2009. - №115(17). – Р. 3842–3845.
- Baxter E.G., Scot L.M., Campbell P.J. et al. Acquired mutation of the tyrosine kinase JAK2 in human myeloproliferative disorders // Lancet. – 2005. - №365(9464). – Р. 1054–1061.
- Bench A.J., Nacheva E.P., Champion K.M., Green A.M. Molecular genetics and cytogenetics of myeloproliferative disorders // Baillieres Clin Haematol. – 1998. - №11. – Р. 819–848.
- Bornhauser M., Mohr. B., Oelschlaegel U. et al. Concurrent JAK2V617F mutation and BCR-ABL translocation within commited myeloid progenitors in myelofibrosis // Leukemia. – 2007. - №21(8). – Р. 1824–1826.
- Kralovics R., Passmonti F., Busser A.S. et al. Again-of-function mutation of JAK2 in myeloproliferative disorders // N Engl J Med. – 2005. - №352. – Р. 1779–1790.
- Levine R.L., Wadleigh M., Cools J., Wlodarska I. et al. Activating mutation in the tyrosin kinase JAK2 in polycythemia vera, essential trombocythemia and myeloid metaplasia with myelofibrosis // Cancer Cell. – 2005. - №7(4). – Р. 387–397.
- Reilly J.T., Snowden J.A., Spearing R.L. et al. Cytogenetic abnormalities and their prognostic significance in idiopathic myelofibrosis: a study of 106 cases // Br J Haematol. – 1997. - №98. – Р. 96–102.
- Spivak J.L. The chronic myeloproliferative disorders: clonality and clinical heteroheneity // Semin Haematol. – 2004. - №41(3). – Р. 1–5.
- Tefferi A., Mesa R.A., Schroeder G. et al. Cytogenetic findings and their clinical relevance in myelofibrosis with myeloid metaplasia // Br J Haematol. – 2001. - №113. – Р. 763-769.