History:
Kazakhstan is a country with a rich historical and cultural past that can be partially explained by geographical location of the country in the very heart of Central Asia at the crossroads of diverse liaisons between European and Asian civilizations - cultural and political, social and economical. At different stages in its history the area of the contemporary Kazakhstan witnessed evolvement, formation and complete disappearance of immense empires and states that would leave an undeniable trace and impact in the world history.
The second half of the XVth century was marked by the process of consolidation of the great steppe nomads into one amalgamated ethnicity that occurred to be the set out of the Kazakh people and the state itself. The nomadic cultures of the steppe presented numerous ethnic substrates that nevertheless shared ancestry, mode of life and history. Since antiquity historical origins of the Kazakh people and all the nations that ever populated the area appear to be part and parcel of the world history, having a powerful impact on the civilizations of Europe, Asia, Africa, the Mediterranean and the New World.
Ethnically and historically Kazakhs belong to the group of the Turkic peoples and rate fourth largest nation among them, besides the fact that immense territory of the country won it a place amid the top ten largest countries across the globe. Demographically Kazakh rate 70th among the two thousands ethnicities and nations. The republic of Kazakhstan currently registers over hundred nations and ethnic groups permanently residing in it [1].
After the collapse of the USSR, Kazakhstan has declared it political and economical independence. Today Kazakhstan occupies the area of 2.7 million square kilometers, thus rating the ninth largest country in the world. The country is geographically situated between Russia and China, and borders on Kyrgyzstan, Uzbekistan and Turkmenistan[2].
Once the giant Soviet super-empire collapsed, Kazakhstan naturally inherited a powerful nuclear weapons arsenal rating fourth biggest in the world, yet the government has resolved not to pursue development of the nuclear weapons for the sake of peaceful relations equally with all the political partners across the world. Political System:
Kazakhstan has chosen path to sovereign democracy and pursues it. It is a unitary secular state with the presidential form of government, priority of the Constitution and legislative system, the government and a parliament comprising two houses. The power of the State is one and governs all in accordance with the Law of Constitution. The state government is duly diverged into three branches: legislative and judicial; their interaction as well as the system of checks and balances as the governing principles of the state.
The country is divided into sixteen administrative units - fourteen districts and two main cities. Astana is the capital since 1997, its population reaches 700,000 people. Since the city has been ascribed its current political status, intensive construction has by far extended the city, naturally located in the steppe, making it into one of the most beautiful metropolis of the Central Asia.
Almaty - the former capital of the country - today rates the second financial and cultural hubbub. Its population is above 1.5 million people [3].
Economics:
Country has won its independence and that would naturally give start to many processes evolving in diverse spheres of the country's life. The country has won its independence , yet for some time would bear the shackles of most distressing economical crisis, that required effective marketing system to recover and recuperate financial and credit foundation and sufficiently heighten the productivity of all industry. Economical reforms that boosted privatization of industry, land and enterprises, gradual evolvement of entrepreneurship and, most important, search for economic liaisons with foreign investors - made the headway for the country's economic strategy.
Year 1993 marked the first step to stabilize the financial system - national currency was changed to Tenge, and hence currency and bank credit system was taken under absolute control of the state. The result would be almost immediate - in 1995 inflation would be reduced to 4%. Towards the end of 1996- beginning of 1997 productivity of all industry was sufficiently raised and retained. Gross Domestic Product (GDP) has grown sixty two times more within the twenty years of country' independence (1991 -2011) - from 2.93 billion $ (in 1991) to 188 billion $(in 2011) [4].
2003, May 17, Kazakh Government has adopted a new “Strategy of industrial and innovative development of Kazakhstan 2003 -2015” that has to fundamentally secure current growth and gradually shift the emphasis on natural resources to industrial preference.
President Mr. N.A. Nazarbayev has explicitly stressed that the strategy would secure entrepreneurship, business initiative and evolvement of small businesses. The strategy suggests active support on behalf of the state inner policy, advance of scientific research and hi-tech innovations. Financial and credit system will be accordingly altered and customized to provide matching taxation and educational basis, as well as antimonopolistic preferences of the economic infrastructure. Accordingly, the highest world standards would be introduced into all the branches of economics and hence Public Health Care would gain from the strategy [5].
Demographic Situation:
Recent polls registered 16, 911 000 people residing in the country. Among them 9, 264 000 live in the metropolis and 7, 646 000 - in the countryside. Life expectancy at birth made 69.57 in year 2012, (compared to 66 in 2002 and 66.38 in 2007). Higher quality of public health care and definitely better standards of living caused by economic stability by 2012, life expectancy at birth increased by 3.19 years and made 69.57 years. In comparison to the EU countries our life expectancy at birth is relatively low. Among the reasons of death of the adult population in the country stroke, cancer, ischemic heart disease, tuberculosis and diabetes are the most frequent. Ecological pollution in some of the country's regions, air pollution in the metropolis area rate among the first risk factors for some of the above-mentioned diseases. Poor information on healthy mode of life and on preventive medicine, poor water-supply quality in some of the districts and inclement climate, as well as destitution of financially insecure strata of the population add to the insufficient quality of public health. One of the main factors must be unsatisfactory state of preventive medicine within the framework of public health care, i.e when we aim at preventive measures against the common diseases among the population, instead of curing the diseased patients.
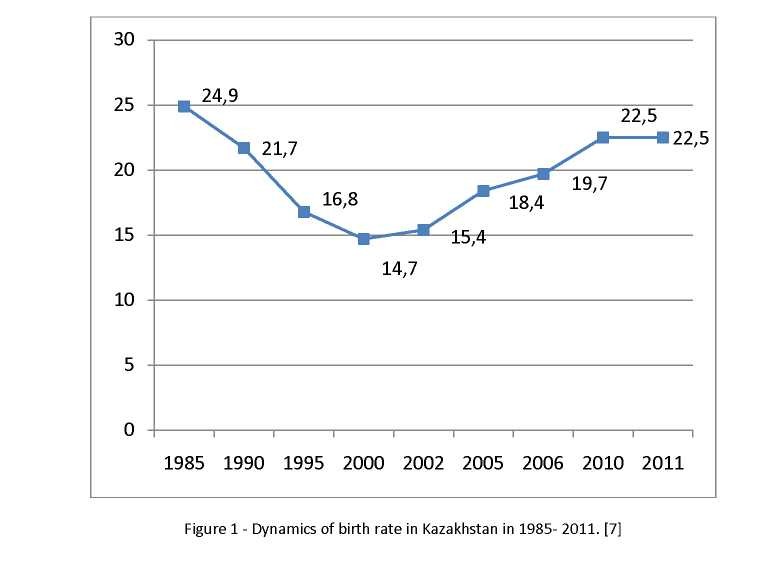
Natality rate is positive and after a definitive fall of 1990s, it is constantly increasing approaching the rate of 1985. In 1985 natality rate made 24.9 per 1000 people. In 2012 birth rate grew by 8. 41% to 22.58 per 1000 people, compared to 2007 when it was only 20.79 per 1000 people. Death rate has accordingly decreased by 17.7 % : it was 10.22 per 1000 people in 2007, and 8.41 per 1000 in year 2012. In year 2007 natality rate made 10.57 per 1000 people [6].
Health Public Care in Republic of Kazakhstan
History of Kazakh Public Health Care:
Soviet public health care was the only system that could be existent in all the republics after collapse of the country. Efficiency of the health care was considerably revalorized in the period following 'perestroyka' (re-formation of the political hierarchy and social values). The existent public health care was excessively grand in its scope, its diverse branches were poorly linked and had little collaboration, hence many functions had to be doubled. Clinical health care was disproportionately emphasized within the framework of the system, and therefore made it quite expensive. Malfunction of its administrative management, ill-use of its human resources and poor finance made the system collapse.
Many inconsistent and abrupt attempts were taken to reform the system in the first years of country's independence, yet they would persistently fail due to lack of proper analysis. Insufficient human resources and frequent (not always logical) alterations in structure and administration of health care seemed to cause malfunction of the whole system. None of those reforms answered the demands of the contemporary needs of the population for various objective and subjective reasons: insufficient funds, outdated facilities, unmotivated (economically and otherwise) medical staff, consumerist approach to one's health permanently established in one's education and mind. But it had to be overcome.
Current health care system:
Period of political and economical stability paved way for due and efficient reforms in public health care (PHC) within six years 2004 till 2010 the overall budget of the PHC was gradually and constantly increased. Yet mere expansion of PHC budget would make an extensive model of PHC that has been proved to be less efficient. Therefore reformation had to be complex and at all the levels: technical and intellectual facilities, infrastructure and management had to be altered and modernized. Evidence -based medicine and know-how approved by the WHO (World Health Organization) were adopted as the new principles [8].
The first step towards better Public Health Care was to adopt a "State Programme of Reforms in PHC in Kazakhstan 2005-2010" and a "Health Codex" in 2009 that would be an all-inclusive alteration and construction of a high quality PHC and medical service in the country. 2010 a unified conception of "National system of the PHC of Kazakhstan" insured every single citizen with a free choice of General Practitioner (GP), specialized doctors and medical services provided by medical organizations. The conception would finally seal competitive basis for all the medical services valued by their final outcome. Thee step by step programs can boast today significant achievements in the field of Medical Services and PHC:
- Granting free medications on the basis of measured benefits and discounts;
- Division of PHC into a network of clinics and branches;
- Advanced facilities and Foundation of an independent medical expert committee;
- Educational and qualification courses for the administration and management staff of the PHC;
- Wide application of "Unified Pharmaceutical System Distributing Medications" across the country;
- Most updated high-tech facilities and video-control systems across the country's clinics;
- Foundation of a National Republican Information Centre for Analysis and Monitoring;
- All the medical schools and colleges are on self-cost economical management;
- Establishment of evidence-based medicine centers in all Medicine research centers across the country;
- State control of the medications' costs. By the moment there has been reached a considerable discount of 30% [9].
Some problems have been left then quite unsolved: for instance legislative lack of responsibility of the state, an employer and a citizen for his/her health state, medical insurance still needed modernization. The state program "Health Codex" of 2009 sought to apply overall medical insurance. Yet scope of medical insurance would be relatively minimal by 2010 - 1.8 % people had been insured. Awareness of require medical insurance was rather insufficient for the medical insurance companies to be stimulated and to advance the market of medical services offered in the insurance policy. Private medical insurance is to be evolved and developed along the state provision of subsidized medical insurance. The idea of medical insurance suggests decreasing the quantity of unplanned costs on medical services - for the citizens as well as for the state, i.e. for the taxpayers. Besides properly arranged medical insurance motivates clinical management, nurses, general practitioners and doctors to offer high quality services and cut the costs of unnecessary or unjustified tests and procedures. Private medical insurance is spread mainly among the companies offering it as part of a contract package to their employees. Whereas assistance companies and clinics have not yet developed necessary liaisons marketing their services to the wide public. Insurance covered by private medical assistance companies is significantly lesser than the coverage of medical services provided by so called state free insurance - 'guaranteed provision of medical services'. We should search for and adopt the ways of motivating and increasing private and obligatory medical insurance. The example of other countries where like in Israel over 80% of the
population is covered by private insurance, might be useful. Modern Kazakh PHC is a medico-social oriented model. The main medical organizations actively involved in PHC are stationary hospitals and ambulatory centers of first medical and sanitary aid. State covers 70-80% of the stationary hospitals expenses. This specific system of insuring stationary hospitals heavily depends on state budget and is certainly expensive. So far, if we intend to transform and modernize it, medical insurance and social insurance have to be set apart, as two diverse kinds of insurance. Next step is to separate between provision of social insurance and the medical services offered and covered by the Public Health system. That would allow finding new ways to significantly lessen heavy load of state subsidies on PHC in Kazakhstan. Such separation of two blocks of insurance - social and medical - would let us evaluate the amount of purely medical expenses on stationary hospitals that certainly would order somewhat coalesced notions of health insurance in PHC. Transformation of our current PHC system to the world standards of medical insurance and medical services to the population would be then more plausible.
Revision of medico-social stationery hospitals' model would let us, similarly to European experience, separate and withdraw the social insurance managers from the administration of the hospitals, where they and their branch of insurance services do not belong.
So far, reformation of contemporary Kazakh Public Health Care system must be done in a complex of scientifically based analytical legislative schemes that would consider country's cultural and spiritual traditions - for the sake of state's and people's interests [10].
Human resources:
"State Programme of Reforms in PHC in Kazakhstan 2005-2010" has taken considerably improved the quality of human resources trained for the advanced and re-formed PHC. The basic requirements for the medical and pharmaceutical education were established and approved of by the law and by the medical schools and colleges. Starting with 2007 the Highest Board of Academic Education has adopted modernized and updated curriculums for the medical schools and colleges. So far, recent graduates would be armed by the last know-how facilities and the experience of the world's best medical research centers.
As the result of reformation, state subsidized Medical schools purchased updated clinical and laboratory facilities for the students. 85% of medical colleges acquired a new economical status of selfmanagement, enjoying independence of decision making for the first time.
Medical schools gain from introduction of new educative innovations. New educative clinical centers provide ample ground for the clinical work required for any medical student and interns. Ways of professional and educative attestment of the teaching staff and of the graduates are set a new, based on the global standards of quality of the World Federation of Medical Education.
Overseas qualification courses for the working medical staff have been one of the major focuses of the state program. Another innovation was to invite known experts in diverse spheres of medicine to lead master classes in Kazakhstan. For instance the program has facilitated close collaboration of medical schools and colleges of Kazakhstan and university centers of Israel. Israel invited many of Kazakh medical experts and doctors of Medicine to participate in qualification courses in its university centers. Doctors of Medicine from Israel took part in Kazakhstan based projects teaching students and sharing their experience with the professors' staff of the Kazakh universities and research centers. Human resources is nevertheless a problematic issue for the Kazakh PHC system.
Today the Medical field registers approximately 59,ooo doctors and general practitioners (GP). Yet there is a considerable shortage of certified medical staff in rural area, despite annual increase of certified graduates of medical schools (over 9.5 % each year). Medical staff in the rural areas is four times less than in the metropolis. It is evident that certified doctors are dispersed across the country's districts extremely unevenly: some districts (Almaty DC) register 9.5 doctors per 10,000 people, others (Karaganda DC) would have twice more - 19.3certified doctors per 10,000 people. Existing and working resources are ageing yearly despite the stream of young experts joining the army of the certified doctors; they make only 4 % [11].
State Subsidies of the PHC:
State subsidies of the Kazakh PHC come from the sources of:
- state budget;
- private medical insurance funds;
- paid medical services;
- other sources that are allowed by the law of Kazakh PHC.
The budget for the so called state 'guaranteed provision of medical services' insurance is granted in accordance to the Main Law of the Republic [12]. Perspectives of further development of Kazakh PHC
Kazakh government has prepared and adopted a programme "Salamatty Kazakhstan" ("State Programme of Future Perspectives of the National PHC in 2011- 2015"). The programme would accentuate sharing responsibility for the health care by direct financial participation of employers and employees.
The programme aims at solving the most pertinent issues, e.g. problems of inequality in PHC, need to ease the financial load of 'guaranteed free provision of medical services' (per capita), inaccessibility of modern hi-tech facilities for the rural patients that make 45 % of the country's population. The programme's utmost goal is to improve the health of the country's population and thereby facilitate stable social and demographic development of the Republic.
Among the immediate goals set by the programme are:
- Better correlation of diverse ministries and branches of the power that are in charge of the PHC and crucial achievement of sanitary- epidemiological stability (no epidemic or pandemic diseases).
- Further development of "Unitary National System of PHC".
- Perspective advance of medical and pharmaceutical education, advanced scientific research in medicine and pharmaceutics.
- I must note that since the outset of the programme there is definite tendency to improvement in Public Health Care of the Kazakhstan [13].
Conclusion:
Constant improvement of Public Health Care is the best expression of stable national economics and prosperity of the Kazakh people, hence it is number one priority of the Republic government. Transformed and updated PHC system will be well-developed and socially-oriented. High quality of medical services and facilities will be accessible for all the social strata and in all the districts of the country. The new innovative policy in the transformation of the PHC must seal the defined principles of the self-advancing system for the sake of the people's health and prosperity [14].
REFERENCES
- The History of Kazakhstan // Almaty: 2007
- Kuldzanov M. Public Health Care Systems // Times of Change, volume 14 (4). - 2012.
- internet site: www.wikipedia.org
- Three Post Soviet Models of PHC, part two. - Almaty- Bishkek- M.: 2012
- "The strategy of innovative industrial development of Kazakhstan 2003-2015"
- The acheivement of PHC, "Health and Ecology" monthly edition, May 23, 2013
- The Register of Statistics of the Republic of Kazakhstan 1985-2012
- Public Health Care Systems, Times of Change, Kuldzanov M., volume 14 (4), 2012.
- The State Programme of PHC Reforming 2005-2010
- Three Post Soviet Models of PHC, part two, Almaty- Bishkek- Moskva, 2012
- Human Resources in Medicine, Almaty, 2010
- The Law codex of Republic of Kazakhstan "Public Health and the PHC System", 2009
- "State Programme of Future Perspectives of the National PHC in 2011- 2015 Salamaty Kazakhstan"
- Akanov A.A., Kyrakbayev K.K., Chen A.N., Akhmetov U.Y. PHC organisation in Kazakhstan // Astana - Almaty: 2006. - Р.231.