In the review article the basic structures and peculiarities of water and salt metabolism of kidneys, the normal development of the growing organism, the impact of the environment and habitat as well as the effect of the physical and chemical composition of daily drinking water. Kidneys ensuring the release of up to 80 % of water-soluble products formed in the process of metabolism and exogenous substances, are involved in regulating the stability of the concentration of osmotically active substances (osmoregulation), the volume of body fluids (volumetric regulation), the concentration of individual ions (ion regulation) and acid-base equilibrium, being thus the main homeostatic organ. Along with this, the metabolic role of kidneys is shown in the metabolism of proteins, fats and carbohydrates, as well as their importance in the synthesis of biologically active substances and hormones affecting erythropoiesis, blood pressure regulation, calcium metabolism, etc. Only one kidney function will be discussed — its participation in the regulation of water-salt homeostasis in children of different ages. There are many factors that prevent this complicated process from developing normally in young children, particularly in hygienic and sanitary levels. In this regard, currently the infectious diseases of the urogenital system are especially prevalent in young children.
Human body, along with organic substances (proteins, carbohydrates, lipids) contains inorganic substances — water and nutrients that are not sources of energy, but their role for the life of the body is quite important. The concepts of water-salt and mineral metabolism are ambiguous. As known, 65 % of the human body consists of water, and even a small loss of water leads to serious health problems. Hygienic water inventory is not limited to its physiological role. A large amount of water is necessary for sanitary and household purposes. Water can play a hygienic role only if it has the necessary qualities that are characterized by its organoleptic properties, chemical composition and nature of the microflora. Now tap water contains chemical, organic and other compounds and cannot be considered drinking without prior purification. In the territory of Kazakhstan, almost all reservoirs are subject to anthropogenic and technogenic influence. The presence of salmonella, pathogenic Escherichia coli, Vibrio cholerae, viruses and many other pathogens in the water can lead to intestinal diseases; in addition, the risk to human health is associated with the presence in water of toxic chemicals (phenols, petroleum products, compounds of copper, zinc, iron, cadmium, cobalt, molybdenum, arsenic, nickel, lead, dichlorodiphenyltrichloroethane, nitrates, nitrites, formaldehyde, chlorine, cyanides, fluorides, etc.), exceeding MPC. Extremely high levels of water pollution are noted in different regions. The predominant pollutants of water reservoirs are phenols, petroleum products, easily oxidized organic compounds, surfactants, nitrates, nitrites, iron, copper, manganese, and zinc. Although it complies with all hygienic standards, these elements in the water will inevitably lead to many infectious diseases, which can adversely affect the normal functioning of the water and salt circulation in the kidneys after entering the body of young children [1].
Methodology
The tissues and organs of a child's body contain significantly more water than an adult. At birth, the water content is 80 %, children of the first five years contain 70 % of body weight. During physiological weight loss (in the first days after birth), the child loses water (8.7 % of body weight) by evaporation during breathing, from the skin surface, with urine and meconium. Removal of water by evaporation is 52–75 % in total. Children have a large body surface and kidney immaturity [2]. Extrenore water loss in children is 1 ml per 1 kg of body weight per hour (for adults — 0.45 ml/kg). Water loss by perspiration is up to 30 ml/kg. With age there is a change in the content of intracellular and extracellular fluid (Table).
Table
The content of the total amount of water (%) and the ratio in the distribution of the liquid depending on age
|
Indicator |
Newborn |
1-6 months |
6 months -1 year |
1-5 years |
Adult |
|
Total amount of water |
75-80 |
70 |
70 |
60-65 |
60-65 |
|
Intracellular |
30-40 |
30 |
35 |
35-40 |
40-45 |
|
Extracellular |
|||||
|
Interstitial |
32-44 |
34,5 |
30 |
25 |
17 |
|
Plasma |
6 |
5,5 |
5 |
5 |
5 |
Physical and chemical properties of water. The main functions of water in the body.
- An indispensable nutritional factor (a person dies after losing 12-25 % of water).
- Universal solvent of organic and inorganic substances (being a neutral medium, water does not alter the chemical properties of the substances dissolved in it; ensures their dissociation and thus the activation of a number of biomolecules).
- The basis of the internal environment of the body (2/3 of the body weight of an adult is water).
- Structural component of tissues (most functioning tissues contain more water).
- Takes part in the structural organization of biomembranes and their bases — a double lipid layer in which the hydrophilic surfaces of each monolayer interact with water.
- Performs the role of hydrate shell of biopolymers and cellular organelles (for example, the interaction of water with proteins ensures their conformation).
- Transport role — the transfer of substances both within the cell and in the surrounding extracellular space, between the organs.
- Participation in biochemical reactions (hydrolysis, redox).
- Regulation of osmotic pressure (isosmia).
- Maintaining body temperature (isothermia); water evaporation by the skin is a device for maintaining a constant body temperature.
- Maintaining the ion environment (рН).
- Mechanical (weakens friction between articular surfaces, ligaments, muscles) [2, 3].
Results and discussion
Features of children's water-salt metabolism. A distinctive feature of water-salt metabolism of young children is greater release of water with exhaled air (in the form of water vapor) and through the skin (up to half of the total amount of water introduced into the body of a child) compared to adults. Water loss during breathing and evaporation from the surface of the baby's skin is 1.3 g/kg body weight per 1 hour (adults' — 0.5 g/kg body weight per 1 hour). The daily need for water of a child of the first year is 100-165 ml/kg, which is 2-3 times higher than the need for water of adults. Daily dieresis of a child aged 1 month is 100350 ml, 6 months — 250-500 ml, 1 year — 300-600 ml, 10 years — 1000-1300 ml. In the first year of a child's life the relative value of its daily dieresis is 2-3 times higher than that of adults. In young children the so-called physiological hyperaldosteronism is noted, which is obviously one of the factors determining the distribution of intracellular and extracellular fluid in the children's body (up to 40 % of all water in young children falls on extracellular fluid, about 30 % — on intracellular, with a total relative water content in the body of a child 65-70 %; in adults, extracellular fluid accounts for 20 %, intracellular — 40-45 % with a total relative water content of 60-65 %. The composition of electrolytes of extracellular fluid and blood plasma in children and adults do not differ significantly, only in newborns there is a slightly higher content of potassium ions in the blood plasma and a tendency to metabolic acidosis. Urine in newborns and infants may be almost completely devoid of electrolytes. In children under age of 5, excretion of potassium in the urine usually exceeds sodium excretion, by about age of 5, the renal excretion of sodium and potassium levels out (about 3 mmol/kg body weight). In older children, sodium excretion exceeds the excretion of potassium: 2.3 and 1.8 mmol/kg body weight, respectively. When breastfed, the child of the first half of year receives the right amount of water and salt from mother's milk, but the growing need for minerals makes it necessary to introduce additional quantities of liquid and complementary foods as early as the 4th-5th month of life. While treating intoxication in infants, when a large amount of fluid is injected into the body, there is a risk of water poisoning. Treatment of water intoxication in children is not fundamentally different from the treatment of water intoxication in adults. The system of regulation of water-salt metabolism in children ismore labile than in adults, which can easily lead to its disturbances and significant fluctuations in the osmotic pressure of extracellular fluid. Children react to restriction of drinking water or excess salt intake with the so- called salt fever. Hydro ability of tissues in children determines their tendency to develop a symptom complex of dehydration (exsicosis). The most severe disorders of water-salt metabolism in children occur in diseases of the gastrointestinal tract, neurotoxin syndrome, and adrenal pathology. In older children, water-salt metabolism is particularly severely disturbed by nephropathy and circulatory failure [4, 5].
Body's need for water. The body's need for water depends on: age, intensity of metabolic processes, physical activity, the functional state of the kidneys, body temperature and the environment, the nature of nutrition. Absorption of water occurs throughout the gastrointestinal tract, most of it is reabsorbed in the small intestine. The main ways of entry and removal of water from the body are shown in Figure.
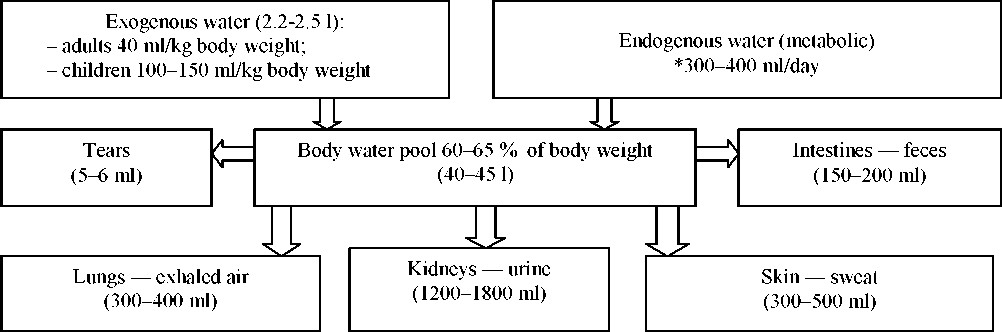
Figure. The main ways of entry and removal of water from the body are shown, body water pool
The amount of endogenous (metabolic) water depends on the nature of the decomposing substrate: thus, upon oxidation of 100 g of fat 107 ml of water are formed, 100 g of protein — 41 ml of water, 100 g of carbohydrates — 55 ml of water.
In childhood, water metabolism is more intense than in adults. In young children, there is a high permeability of cell membranes, and the fixation of fluid in the cells and the intercellular space is weak. In a child, the volumes of chloride (extracellular water) and inulin space (labile water) are almost the same and make up 41 and 40 % of body weight, respectively (in an adult — 26.4 % and 16 %).In children, water metabolism is labile due to the mobility of extracellular water. During dehydration (loss of fluid) there is a significant decrease in both extra-and intracellular fluid. The children's need for water is much higher than in adults: from 10 days of life to 5 years is 130-150 ml/kg body weight.
Sodium. The sodium content in the serum of the newborn is the same as in the mother's blood (≈ 142 mmol/l). The intracellular sodium content in children is higher, which is associated with the maturation processes of the «sodium pump» in the cells.
Potassium. In newborns, the potassium content is up to 6.6 mmol/l. The content of potassium in the blood of more than 6 mmol/l is dangerous for the life of children older than 1 month. Daily need for potassium is higher than in adults. The lack of potassium in the children's body retards the growth and development of the child.
Calcium. Enters the fetus transplacentally through active transport. In the last months of pregnancy, up to 100-150 mg of calcium per kg of fetus weight is daily supplied. The body of the newborn contains 30 g of calcium. Up to 4 months there is a rapid growth and mineralization of bone tissue. To ensure this process, the child needs to receive 500 mg of calcium daily. The children's body of the first year contains calcium of 400 mmol/kg body weight. The calcium content in the blood of full-term newborns is 2.25-2.45 mmol/l, the first year and older is 2.5-2.8 mmol/l. In healthy children, 0.1-0.3 g/day of calcium is excreted in the urine; much of it is excreted with feces.
Magnesium. Every day, the fetus receives 3-4 mg of magnesium. The concentration of magnesium in serum is 0.66-0.99 mmol/l, 2/3 of magnesium is in ionized form. Hypomagnesaemia in children is manifested by increased neuromuscular excitability, prolonged diarrhea. Hypomagnesaemia is observed in children receiving large doses of vitamin D.
Phosphorus. Enters the fetus against the concentration gradient. The concentration of phosphorus in the blood serum of the first year child is 1.29–2.26 mmol/l, from 2 to 4 years — 0.65–1.62 mmol/l.
The age-related features of calcium, magnesium and phosphorus metabolism are determined by the state of the neuroendocrine regulation of homeostasis and bone tissue mineralization.
The effect of ant diuretic hormone and aldosterone on the body of a child of the first year is significantly less expressed than in children older than 1 year.
Humoral regulation and violation of water-salt metabolism. The main hormones involved in the humoral regulation of water-salt metabolism are ant diuretic hormone, aldosterone, atrial natriuretic factor and rennin — angiotensin system.
Ant diuretic hormone (vasopressin). It is synthesized in the supraoptic and paraventricular nuclei of the hypothalamus, it is transported to the neurohypophysis a long the supraopticohypophysial tract, from which it is secreted into the blood. By chemical nature, it refers to the hormones of the protein-peptide nature, it is a nanopeptide. Target organs are vessels, distal tubules of the kidneys. The mechanism of action is membrane- intracellular. It is responsible for osmoregulation and fluid volume, regulates water balance, has a vasoconstrictor effect, regulates the functioning of the cardiovascular system [6].
Effects of ant diuretic hormone (ADH):
- ant diuretic hormone (interacts with V2-receptors in the renal tubules, increases the level of cAMP, phosphorylates proteins, increases the permeability of membranes to water and its reabsorption):
Increase of osmotic pressure of blood plasma
↓ Excitation of osmoreceptors of the hypothalamus
↓ Secretion of ADH from secretory granules
↓ Distal tubules of the kidneys (Activation of hyaluronidase)
↓ Hyaluronic acid depolymerization
↓ Increase of permeability of the distal water tubules
↓ Decrease of diuresis (water is retained in the body)
- regulation of blood pressure (interacts with V1-receptors of smooth muscle cells in blood vessels, increases the concentration of calcium in the cells, causes muscle contraction, vasoconstriction and high blood pressure);
- participates in memory mechanisms, namely in fixing memory, mobilizing information.
Conclusion
Kidney and urinary tract diseases are common in children. The main contingent of the neurological department — patients with infection of the urinary system (pyelonephritis, cystitis); children suffering from glomerulonephritis, interstitial nephritis, disorders of water-salt metabolism. An important part of the treatment of diseases of the kidneys and urinary tract are diet, water and salt regimen.
The problem of urinary tract infection (UTI) in children continues to be one of the most pressing in pediatric nephrology, since this group of diseases takes first place in the structure of nephropathy, significantly exceeding the prevalence of glomerulonephritis and other kidney damages. In the early 90s of the last century, UTI was considered to be the main unrecognized threat to a child's health, since the latent course of pyelonephritis (PN) was found in 2–20 % of cases, and asymptomatic bacteriuria — in approximately 1–2 % of healthy girls. These data led to the excessive use of invasive methods of diagnosis and treatment of UTI with the aim of preventing the development of chronic renal failure. Over the past two decades, circumstances have changed. Currently, it is considered that only some cases of UTI are a serious or life-threatening problem; surgical treatment is indicated for a small number of children with recurrent UTI and structural urinary tract anomalies that can be surgically corrected.
At the present stage, the problem of urological infections is one of the big issues, because of the tendency to increased frequency of diseases of the urinary tract.
Peculiarities of urinary tract infections are determined not only by medical but also by socio-economic significance of the problem.
The causative agent of urinary tract infections is microflora colonizing the periurral area. They are mainly conditional-pathogenic microorganisms belonging to the family of enterobacteria, including the intestinal stick which is the first.
References
- Elpiner, L.I. (2016). Mediko-ekolohicheskie podkhody k intehralnomu upravleniu vodnymi resursami [Medical and environmental approaches to integrated water resources management]. Hihiena i sanitariia — Hygiene and sanitation, 2, 5, 15-18 [in Russian].
- Kuznetsova, A.A., Revnova, M.O., & Natochin, Yu.V. (2015). Vodno-solevoi obmen i funktsii pochek u detei pri tseliakii i khronicheskom hastroduodenite [Water-salt metabolism and renal function in children with coeliac disease and chronic gastroduodenitis]. Pediatriia — Pediatrics. 2, 5, 27-31 [in Russian].
- Aizman, R.I. (2017). Formirovanie funktsii pochek i vodno-solevoho obmena v ontoheneze [Formation of renal function and water-salt metabolism in ontogenesis]. Nauchnyi proekt vozrastnoi Jiziolohii — Scientific project of age physiology, 1, 108-118 [in Russian].
- Ilyin, F.E., & Darinsky, Yu.A. (2017). Ekolohicheskii monitorinh pitevoi i poverkhnostnykh vod Irtysha i Tobola [Environmental monitoring of drinking and surface waters of the Irtysh and Tobol]. Ekolohia cheloveka — Human Ecology, 1, 1, 281-290 [in Russian].
- Gerasev, A.D. (2016). Analiz mekhanizma deistviia tseolita Shivyrtuiskoho mestorozhdeniia na vodno-solevoi obmen i funktsiiu pochek [Analysis of the mechanism of action of zeolite of the Shivyrtuyskoye field on water-salt metabolism and kidney function]. Extended abstract of Doctor's thesis. Novosibirsk [in Russian].
- Aizman, R.I. (2008). Metodika kompleksnoi otsenki zdorovia uchashchikhsia obshcheobrazovatelnykh shkol [Methods of comprehensive assessment of the health of students in secondary schools]. (Vol. 1). Novosibirsk [in Russian].