SUMMARY
This article presents a literature review on the need of preparation patients who has terminal stage of chronic renal failure for the renal replacement therapy - dialysis, and the nurse's role in the pre-dialysis education for these patients and for their relatives. Annually more than 2.5 million people around the world receive dialysis because they have chronic renal failure. Dialysis is a vital procedure. This is explained by the fact that the artificial kidney apparatus helps to purify human blood from toxins and remove excess fluid from the body, that is, it performs the physiological work of the kidneys when they themselves cannot cope with this problem. Chronic renal failure and dialysis procedures are quite serious difficulties for both the patients and their families. First, it depends on the misinformation or complete lack of information of patients, acceptance of the need for lifestyle changes for the whole family, as well as adaptation to the new day regimen and nutrition, etc. In this difficult period, patients and their families need moral support, as well as in obtaining reliable information that, they need to quickly adapt to new living conditions, which, in turn, contributes to the effectiveness of renal replacement therapy.
The nurses are the important actors in the pre-dialysis education of patients. In such situations, one of the most important aspects is to organize the proper care of patients and to ensure compliance with the basic life rules - drinking restriction, dieting, and care for vascular access and so on. This is all are different aspects of caring for such patients. Therefore, the nurse contributes to improving the patients' quality of life by educating and supporting of completely patient is family. A nurse can have different roles i.e. a mentor, a teacher or a coordinator who always can help all of them by providing all the necessary information.
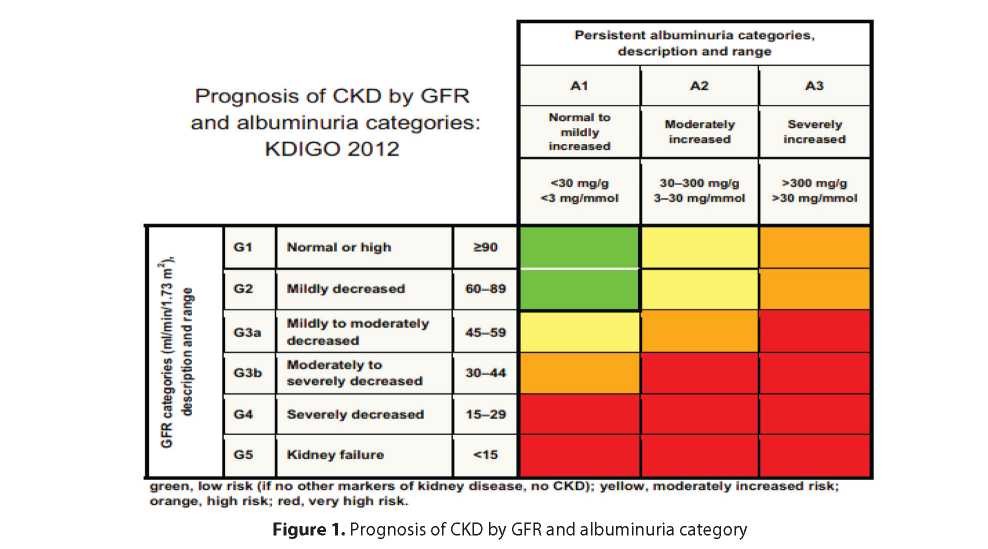
Chronic Kidney Disease (CKD) is defined as abnormalities of kidney structure or function, present for > 3 months, with implications for health. CKD is classified based on cause, glomerular filtration rate (GFR) category (G1–G5), and albuminuria category (A1–A3), abbreviated as CGA [1,2] (Figure 1).
The level of albuminuria is determined on the basis of the daily excretion of albumin in the urine or the albumin / creatinine ratio. A complete diagnosis of CKD contains name of the kidney disease (the cause of CKD, if known) along with the assigned appropriate stage G and A.
CKD leads to the development of renal failure, which in turn leads to a breakdown of the physiological, psychological and social well-being of a person [3].
Chronic renal failure (CRF) is a nonspecific syndrome developed because of gradual loss of major renal functions due to development of sclerosis of the kidney tissue on the background of various progressive kidney diseases. Chronic renal failure is a progressive and irreversible loss of renal function.
Chronic renal failure refers to the stages of CKP G3- G5; Stage G5 is the terminal stage of renal failure or uremia (KDIGO 2017). In the absence of appropriate treatment, the patient slowly and painfully dies.
Most patients have a terminal stage of CKD. At this stage of the disease, the beginning of renal replacement therapy is mandatory. There are several types of RRT. It can be hemodialysis, peritoneal dialysis, and kidney transplantation.
According to the Clinical Protocol of the Ministry of Health of the Republic of Kazakhstan “Chronic kidney disease among adults” (2016), the treatment strategy for patients with stages CKD 4-5 is defined as preparation for renal replacement therapy, adequate dialysis therapy: from the start of dialysis to the achievement of goals, treatment of complications CRF and dialysis therapy.
In this case, chronic kidney disease and subsequent hemodialysis cause a number of problems in different aspects of life (social, psychological, cultural, spiritual) of patients and their families [4].
Hemodialysis is a process that removes toxins from the blood and excess fluid, provided that the kidneys can no longer perform their function. This is a method of additional purification of the kidneys from substances with low and medium molecular weight by diffusion and partial convection (ultrafiltration) through an artificial semi-permeable membrane. During dialysis, the patient connects to an artificial kidney machine [5]. The order of the Ministry of Health of the Republic of Kazakhstan “On approval of the standard for the provision of nephrological assistance to the population in the Republic of Kazakhstan” [6] identifies the following criteria for the selection and initiation of renal replacement therapy: (the presence of one of the indicators is the reason for the onset of renal replacement therapy):
- Urea of blood serum above 30 mmol / l and / or decrease in glomerular filtration rate (hereinafter - GFR) below 10 ml / min / 1.73 m 2 (in patients with diabetes less than 20 ml / min / 1.73 m
- MDRD/СKD-EPI: 2) GFR (ml / min / 1.73m2) = 186 x (plasma creatinine) -1.154 x (age) -0.203 x (0.742 - for women);
- a decrease in the standard bicarbonate below 20 mmol / l and / or a buffer base deficiency of less than 10 mmol / l;
- Hyperkalemia - over 6.5 mmol / l.
Before starting hemodialysis, vascular access is provided. Blood is taken from the patient's body and returns back through a surgically formed arterio-venous fistula.
The goal of hemodialysis is a long-term life support of renal replacement therapy for persons with terminal stage of chronic renal failure [7].
In accordance with Annex 1 to the standard structure of the Clinical Protocol Chronic kidney disease [7], the standard dose of dialysis - 3 times a week for 4 hours. Within 4 hours, toxins and excess fluid are removed from the body, accumulated two days after the previous procedure. Excessive accumulation of fluid in the body contributes to increased blood pressure and the development of cardiovascular pathology. Also it is necessary to remember about observance of the special diet limiting consumption of salt, potassium (fruit, etc.), phosphorus (dairy products, fish, etc.). All these measures are aimed at ensuring life quality of patients on dialysis.
The quality of human life is based on the following factors: physical, social and emotional. A decline in the quality of life can result from a violation of physical health, psychological health, social relations and the environment [8].
The quality of dialysis patients' life largely depends on the pre-dialysis preparation of the patients. The success of dialysis largely depends on the patient's compliance with the recommended treatment regimen, failure to comply with which leads not only to the development of possible complications of the underlying disease, but in general significantly reduces the quality of life [9].
Nowadays, there are several causes of chronic kidney disease. These include diseases the following: diabetes, hypertension, diseases of the cardiovascular system [10,11]. Over time, these diseases can lead the human body to such a serious condition, when the beginning of renal replacement therapy will be the only treatment option. Chronic renal failure, as a special state of health and a certain lifestyle, and dialysis, as a necessary life-saving procedure, can significantly affect the quality of life of patients [12].
Nursing assistance to dialysis patients is a very important aspect and is determined by the peculiarities of this category of patients. To solve various problems of dialysis patients, it is important to strictly follow the prescribed regimen [9].
A positive impact on patients' quality of life has the knowledge and skills of nurses in the care of patients with kidney disease. [10]. But it should take into account the existence of a relationship of trust between the nurse and the patient to be able to accurately assess the needs of the patient.
Thus, the concept of life quality will come from the position of the patient and his family, and not from the position of assessment of the medical worker. Unfortunately, patients on renal replacement therapy suffer from severe and incurable kidney diseases that led to the onset of dialysis. The procedure for hemodialysis is not always smooth and calm, takes quite a long time, and entails various consequences and complications. In this situation, quality nursing helps to maintain the physical and mental well-being of patients and their relatives.
It is very important to know that often dialysis patients, in addition to their primary kidney disease, also suffer from different kinds of concomitant chronic diseases. This factor contributes to an increased level of emotional stress and fear before beginning of the dialysis treatment. Thus, fatigue can be identified as the most common symptom in dialysis patients [10]. This is due not only to the most debilitating hemodialysis procedure, but also to the fact that people suffer from chronic kidney disease for a long time.
At the same time, fatigue is not the only debilitating symptom in dialysis patients. There are also such conditions as loss of appetite, impaired concentration, swelling in the arms and legs, muscle cramps, itching. All these symptoms can cause stress in a person and adversely affect the patient's quality of life. [13].
There are a number of difficult situations that need to be addressed to the patient: the fatigue and the desire to relax after hemodialysis, while you need to go home; the need to be accompanied by a third party due to ill health; difficulties with their time planning, taking into account the frequency and duration of dialysis; difficulties in managing concomitant diseases, in particular with pain [13].
The main points that patients encounter when starting hemodialysis [14]: lifestyle changes (diet, drinking alcohol, actions, etc.), loss of time (time spent on the road and the procedure itself), suffering of different symptoms (poor health after dialysis, the next day weakness, restless leg syndrome, nausea, muscle spasms, etc.), family and sexual functions (lack of sexual desire, inability to perform household duties), restrictions on work, family support, depending on dialysis, medical advice. Many problems can be solved if the patient and his family are properly prepared for hemodialysis. [10, 11].
Pre-dialysis education helps to reduce the fear of hemodialysis itself, as well as the ability to form a AV-fis- tula in advance and learn how to properly care for it [15]. Training should be conducted both with the patients themselves and with relatives. Full information in preparation for dialysis covers the following aspects: people need to know the causes of the disease, which led to end-stage renal failure, the possibility of replacement therapy, the need to regulate diet, monitoring the general condition [16].
It is important that the sources of information should be not only medical workers, but also other patients, which is very important for newly arrived patients [12, 17]. “Experienced” patients can share their experiences and give some necessary advice on lifestyle, diet, self-control methods. However, most patients at the beginning of dialysis therapy want to know only a little about their condition, because it seems difficult for them to learn a large amount of information and they prefer to learn the new gradually and dosedly [12, 16]. At the first stage, too much information can frighten a person and put him in a state of depression [12], so it is necessary to develop minimum criteria for “beginners”.
During dialysis, the patient must also independently apply various methods of self-control of his condition. However, such methods are not clearly defined in the literature. There are only a few general guidelines that are not entirely suitable for dialysis patients [13, 18]. Patient education should continue and include self-education and self-knowledge of various ways to maintain optimal conditions for comorbid chronic diseases (i.e., control and monitoring of certain options associated with such diseases as diabetes, arterial hypertension), hygiene, sleep, rest and nutrition. [13] Patients rely on the support of their families, but do not want to become a burden for them. Therefore, it is important to encourage patients to learn and develop self-control. Taking into account the active support of families, it is necessary to try to raise public awareness about hemodialysis and educate health care workers about the importance of interaction with the families of patients [14]. However, all family members need a greater understanding of these problems, as they will first be responsible for lifestyle changes and routines for dialysis patients.
Patients with terminal stage of kidney disease are divided into 2 types of information perception: one passively accepts information provided by health professionals; others actively ask questions and look for information in various sources [12].
At the beginning of hemodialysis, patients are faced with specific problems that need to be addressed by patients, their relatives and the health care system as a whole. This includes self-awareness of patients and their learning [10, 11]. Lack of knowledge and understanding of their illness give patients' sense of their own disability [18].
Full awareness of his condition contributes to the involvement of the patient and his active participation in improving the quality life [12]. At the same time, the information provided should be extremely clear and unambiguous in order to avoid conflict situations [11]. Also, one should not forget that it is necessary to train not only the patients themselves, but also members of their families, since with the advent of a dialysis patient in the family, it is necessary to change the way of life for the whole family [14, 19].
According to the official statistics, number of patients with CKD is steadily growing [20]. There are “new” patients, differing in the severity of their illness and needs. Therefore, it is necessary to improve the quality of education delivered to the patients. This education leads to patients' involvement in the treatment process, which makes them more competent to track their emotional and physical states. This, in turn, contributes to the development of self-sufficiency and independence in this category of patients [15].
Unfortunately, this often happens that he dialysis patient is a threat to their own safety. This is due, and due to the following factors: the requirements for personnel (patients are often asked to hurry up), failure to comply with safety rules during dialysis (no limb immobilization with AV fistula, a cover of a visual inspection, etc.) Lack of knowledge and non-participation in care [21].
Lack of knowledge about his illness and lack of participation in the treatment process indicate the unpreparedness of patients for hemodialysis [15, 21]. The emergence of fear and disbelief in the loss of kidney function can aggravate the patient's condition [17].
In preparation for hemodialysis, the nurse plays a central role [22]. A qualified nurse should have critical thinking, know different approaches to solving emerging problems, and help to find the best solution for the patient and his family, help to improve the patient's health and quality of life [19]. Nurse helps to improve the quality of life of patients and their tolerability to the procedure [22]. In this regard, five main roles identified in this connection, that the nurse performs.
A holistic assessment of patients on pre-dialysis prepares for timely referral to hemodialysis, identification of needs, assessment of self-care capacity, housing and social conditions, and patient education. A personal acquaintance with the patient makes it possible to make a holistic assessment of the patient to determine the individual monitoring regime for each patient. Exchange of contact information enables nurse to keep in touch with the patient and answer questions that arise.
A nurse like an educator trains and supports the patient before beginning of the renal replacement therapy. In the new conditions of life, the nurse provides patients and his relaatives with the necessary information about the disease: the process of the disease, the impact on life, the possible consequences, facilitates the patient's adaptation to a new state, to the information received, answers emerging questions about both medical and social aspects. In this role, the nurse has the opportunity to conduct group sessions with patients and their relatives, which significantly reduces the time spent, and also positively affects dialysis patients by meeting with other patients and sharing experiences, communicating with each other.
The nurse trains and monitors the patient's condition, all vital signs, thereby preventing the development of possible complications.
The nurse develops her professionalism by working in a multidisciplinary team with various specialists.
It is necessary to develop every time and improve nurse'e role of in carying for dialysis patients, as this is a complex and creative work that requires constant development of the professional and personal characteristics of a nurse.
The nurse observes the patient in the dialysis unit and becomes reliable source of information, which gives the necessary and useful information. A nurse has an important role in obtaining, understanding and using information. In international practice during dialysis, the patient constantly interacts with nurses, and others healthcare spe- sialists [12].
The nurse has a direct impacting to the patient with kidney disease [23]. Understanding the needs and daily difficulties of dialysis patients helps to every healthcare worker to improve the life quality of dialysis patients [14].
The educated nurse can be involved to the dialysis procedure, and also conducts explanatory work on the main aspects and rules of life with the dialysis, helps to gain new knowledge and necessary skills. This helps to ensure decent level of patients' life quality on replacement renal therapy. The nurse acts as a mentor, educator and guide, who has to help the patients and members of his family adapting to new conditions of life. Recommendations received by them should help to reduce the level of stress and fear, and prepare for the beginning of the dialysis, giving explanations of what needs to be done, what should be observed, the importance of the procedure, care of vascular access, possible complications and consequences, etc. In a word, all these actions have to prepare patients psychologically for the vital procedure of dialysis.
REFERENCES
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2017; 7: 1–59.
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney inter., Suppl. 2013; 3: 1–150.
- Morton, R., Tong, A., Howard, K., Snelling, P., Webster, A. The views of patients and carers in treatment decision making for chronic kidney disease: Systematic review and thematic synthesis of qualitative studies. British Medical Journal – 2010 – 340 – 112p.
- Shahgholian, N., Yousefi, Y. Supporting hemodialysis patients: A phenomenological study. Iranian Journal of Nursing and Midwifery Research – 2015 - 20(5), 626–633p.
- Lindsay, Н., МaсGregor, C., Fry, M. The experience of living with chronic illness for the haemodialysis patient: An interpretative phenomenological analysis // Health Sociology Review. – 2014 - 23(3) - 232–241p.
- The order of the Ministry of Health of the Republic of Kazakhstan «On approval of the standard for the provision of nephrological assistance to the population in the Republic of Kazakhstan» - 2013.
- Clinical protocol of the Ministry of Health of the Republic of Kazakhstan «Chronic kidney disease in adults» - 2016.
- The world health organization quality of life (whoqol) –BREF 2004.
- Alikari, V., Matziou, V., Tsironi, M., Theofilou, P., & Zyga, S. The Effect of Nursing Counseling on Improving Knowledge, Adherence to Treatment and Quality of Life of Patients Undergoing Hemodialysis // International Journal of Caring Sciences. – 2015 - 8(2) - 514-518p.
- Horigan, A., Rocchiccioli, О., & Trimm, D. Dialysis and Fatigue: Implications for Nurses – A Case Study Analysis // Medical-Surgical Nursing. – 2012 - 21(3).
- Hallock, A.An ethical approach to renal replacement decisions in the elderly // Nephrology Nursing Journal. – 2014 - 41(5) - 513-518p.
- Bonner, A. & Lloyd, A. Exploring the information practices of people with end-stage kidney disease // Journal of Renal Care. 2012 - 38(3) - 124-130p.
- Horigan, A., Schneider, S., Docherty, S., & Barroso, J. The experience and self-management of fatigue in patients on hemodialysis // Nephrology Nursing Journal. – 2013 - 40(2) - 113-122p.
- Al Nazly, E., Ahmad, M., Musil, C., & Nabolsi, M. Hemodialysis stressors and coping strategies among Jordanian patients on hemodialysis: A qualitative study // Nephrology Nursing Journal. – 2013 - 40(4) - 321-327p.
- Neyhart, C., McCoy, L., Rodegast, B., Gilet, C., Roberts, C., & Downes, K. A new nursing model for the care of patients with chronic kidney disease: The UNC Kidney Center Nephrology Nursing Initiative // Nephrology Nursing Journal. – 2010 - 37(2) - 121-131p.
- Davison, I. & Cooke, S. How nurses' attitudes and actions can influence shared care // Journal of Renal Care. – 2015 - 41(2) - 96–103p.
- Sondrup, B., Copland, M., Black, A., & Trask, M. Supporting patient choice: An intervention to promote independent dialysis therapies // Nephrology Nursing Journal. – 2011 - 38(6) - 491-497p.
- Canadian Association of Nephrology Nurses and Technologists Journal April–June 2011 - 21(2) - 15-37p.
- Shnishil, A. & Mansour, K. Effectiveness of Nursing Practices Guideline on Nurses Practice at Hemodialysis Units in Medical City Directorate // Journal of Nursing and Health Science. – 2017 - 6(5) - 01-11p.
- Devi, E., Prabhu, R., Sequiera, L., Mayya, S. Identification of Health Problems of Patients Undergoing Hemodialysis Using Self Care Deficit Theory and Application of Nursing Process Approach Care // International Journal of Nursing Education. – 2012 - 4(1).
- Thomas-Hawkins, C., Flynn, L., Lindgren, T.G., & Weaver, S. Nurse manager safety practices in outpatient hemodialysis units // Nephrology Nursing Journal. – 2010 - 42(2) - 125-133p.
- Walker, R., Abel, S., & Meyer, A. The role of the pre-dialysis nurse in New Zealand // Renal Society of Australasia Journal. – 2010 - 6(1) - 5-10p.
- Hopkins, D., Kott, M., Pirozzi, J., Deppoliti, D., Pond, M., Randolph, C., & Côté- Arsenault, D. End-of-life issues and the patient with renal disease: An evidence-based practice project // Nephrology Nursing Journal. – 2011 - 38(1) - 79-83p.