Acute phlegmonous appendicitis is an outstanding topic in medicine. The issue can be approached in terms of diagnosis and the importance of practical surgery. The clinical diagnosis can be supported by macroscopic and microscopic anatomo-pathological diagnoses. The microscopic diagnosis can be established after studying morphological characteristics observed by analogy with microscopic preparations stained by traditional and special methods. Pathological microscopic preparations can be analyzed and compared with histological preparations that display normal appendix. This paper presents some best practice examples. To provide a precise explanation to medical staff, a series of images of microscopic slides were taken from patients for microscopic analysis. The creation of permanent microscopic slides was based on knowledge of the steps required for classical histological methods using standard H&E staining techniques. Samples were taken from patients of both sexes, children under 16 years old, from urban and rural areas. It is important to clarify misunderstood epidemiological features of appendicitis. Perforating and non-perforating appendicitis, apparently, are separate in nature, and since the need for spontaneous resolution of appendicitis is essential. It is important to have better quality reference materials to enable the medical staff to make the correct decision; this paper seeks to add to this area of knowledge. Ensuring that the diagnosis is correct can have important implications for the management of appendicitis suspicion. This must be supplemented with histological assessments together with important personal, heredocolateral antecedents in the patient’s pathological history. For example, determinations of the lymphocytopenia and neutrophil-lymphocyte ratio can predict bacteremia better than conventional infection markers in the emergency department. Histopathological analysis remains important for such determinations.
Introduction
Appendicitis is considered to be one of the most common pathologies at ages 10–20 years. However, this pathology can also occur at any age category, without prior knowledge of the determining or incriminating factors [1, 2]. Studies have shown that appendicitis is more prevalent in males than in females [3, 4]. The exact cause of acute appendicitis is unknown, but it is considered likely to have a multi-factorial determinant. In this context, luminal obstruction, microbial infection, and dietary plus familial factors have been suggested to be common and probably synergistic [5–7]. The diagnosis of acute appendicitis is based on a history and a thorough examination [8, 9]. With phlegmonous and complicated appendicitis, these most likely represent independent entities depending on the hereditary immune mechanisms [10–12]. In context, compared to more complicated diseases, phlegmonous appendicitis seems to depend mainly on local inflammation [6, 13, 14]. Further regarding the paraclinical diagnosis, the blood laboratory test (hemoleukogram) will show any signs of eosinophilia [12, 15]. Studies also show that significant values of myeloproliferative disease appear in the blood, namely eosinophilia and basophilia, which can be found in phlegmonous inflammation [16, 17]. Hence, for paraclinical diagnosis, it is important to clarify the role of C–reactive protein (crp) as an indicator of surgical indication for appendicitis [18–20].
To establish the diagnosis of this pathology, histopathological examinations of appendectomy specimens have been used in this paper [21, 22]. This is done to advance medical understanding and improve diagnoses. In this regard, even when the macroscopic appearance of appendectomy specimens is normal, histopathological evaluation allows for a more accurate diagnosis [23–25].
Experimental
To help the medical staff understand the concerns presented above, a series of images were taken after preparing microscopic slides. For this purpose, the operating parts are intended to provide a pathological anatomy service to aid macroscopic examination for diagnostic purposes. After performing microscopicpreparations, they were examined by performing microscopic analysis. The realization of the permanent microscopic preparations was based on knowledge of the steps required for classical histological methods, using a standard H&E staining technique. The samples were extracted from patients of both sexes, children under 16 years of age, from urban and rural areas.
- — male — urban
Diagnostic. Acute phlegmonous appendicitis on appendicular empyema and with acute peritonitis; Biological product — Appendix
Macroscopic — as usually
Microscopic –– Appendix with fibrinoleukocyte content, wall with acute, dispersed inflammatory infiltrates, areas of wall dissolution, and leukocyte exudates on the peritoneal serosa
- — male — rural
Diagnostic. Acute phlegmonous appendicitis; Biological product — Appendix
Macroscopic –– Appendix 50 mm long, diameter 5–6 mm, whitish serous with purplish areas Microscopic — in preparing samples using h&e staining
- — male — urban
Diagnostic. Acute phlegmonous appendicitis with acute peritonitis; Biological product — Appendix
Macroscopic –– Appendix with a length of 50 mm, thickened, diameter 10–14 mm, covered by pseudomembranes, in retained lumen content
Microscopic — in preparing samples using h&e staining
- — male — urban
Diagnostic. Acute phlegmonous appendicitis; Biological product — Appendix
Macroscopic –– as usually
Microscopic — in preparing samples using h&e staining
- — male — rural
Diagnostic. Acute phlegmonous appendicitis with acute peritonitis Biological product — Appendix Macroscopic –– Appendix 35 mm long, thickened, purplish, with tearing area of the wall Microscopic — in preparing samples using h&e staining
- — male — urban
Diagnostic. Acute phlegmonous appendicitis with acute peritonitis; Biological product — Appendix
Macroscopic Appendix with a length of 50 mm, thickened, diameter 10–14 mm, covered by pseudomembranes, in retained lumen content.
Microscopic — in preparing samples using h&e staining.
Results and Discussion
Figure 1 illustrates Specific epithelium; Adjacent lymphoid formations; The underlying connective tissue.
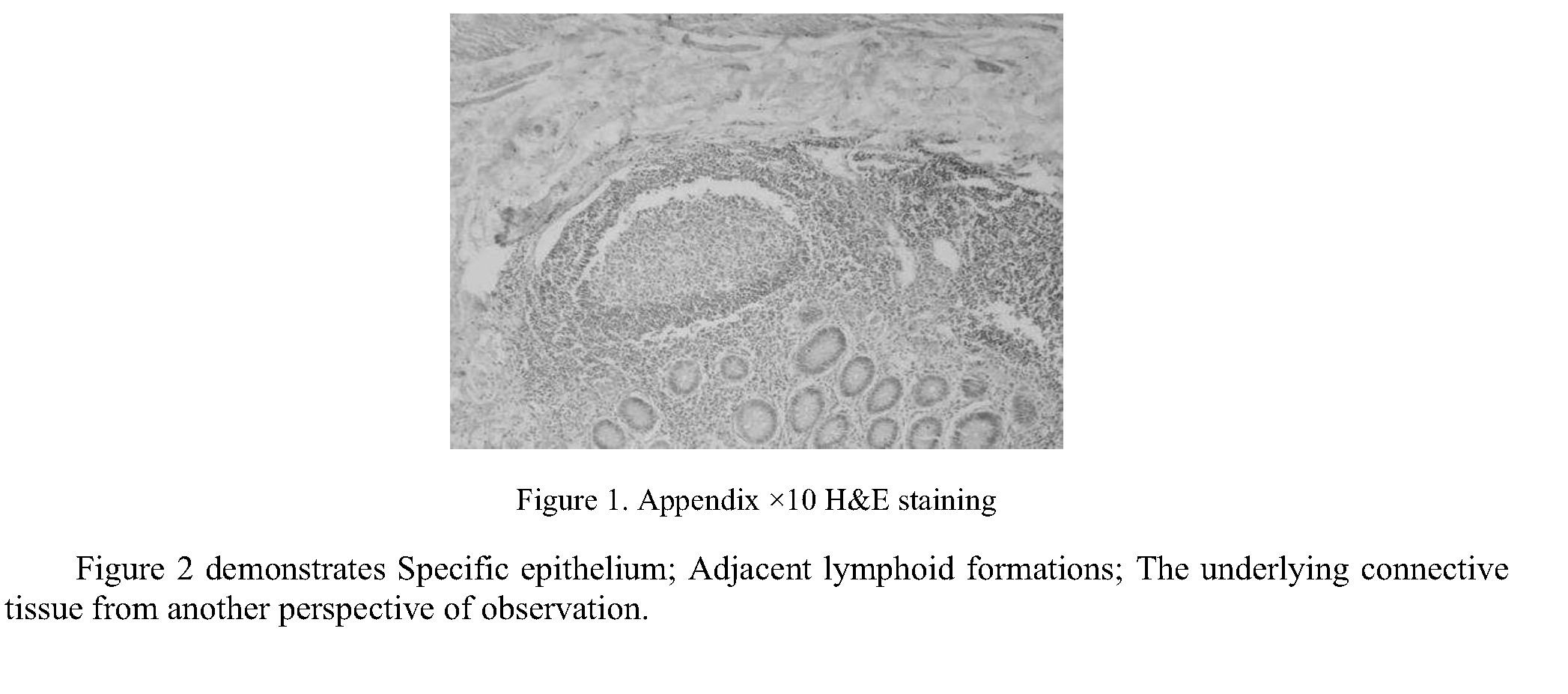
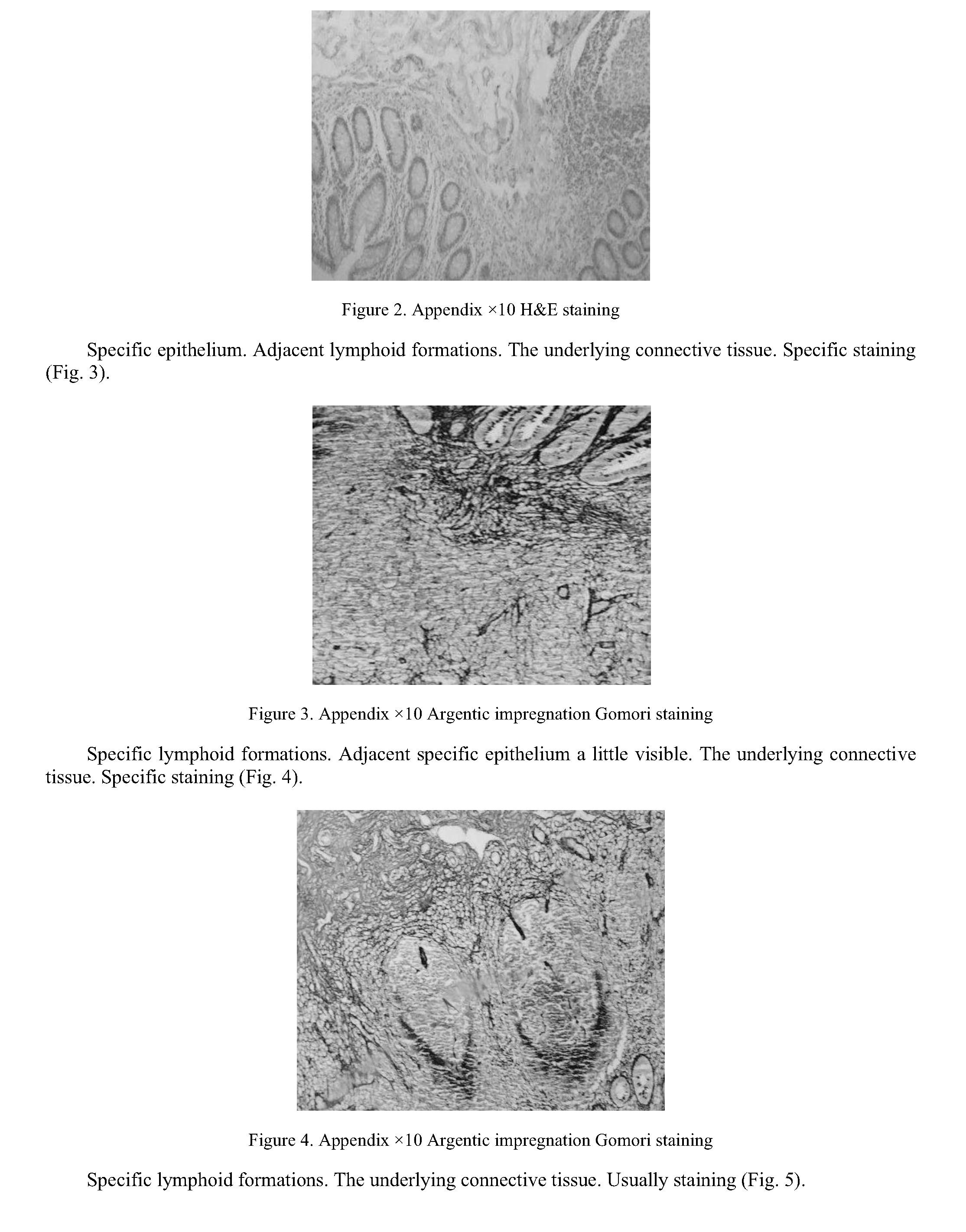

according to the classical histological technique and stained with usual and special stains. From the images with phlegmonous appendicitis, it is noted that appendix changes are variable but characteristic. Macroscopically the appendix appears purple with variable centimeter dimensions. Macroscopically, the appendix may have whitish serosa with purplish areas. Also, from the macroscopic images, the appendix in phlegmonous appendicitis appears thickened, purplish, with the tearing area of the wall. Macroscopically for particular cases presented, the appendix appears covered by pseudomembranes, in the lumen having retained content. There are particular occurrences of acute phlegmonous appendicitis with acute peritonitis. In acute phlegmonous appendicitis on the appendicular empyema and with acute peritonitis, the microscopic appendix appears with specific changes that materialize in the presence of fibrinoleukocyte content, the wall with acute, scattered inflammatory infiltrates, wall dissolution areas, and leukocyte exudates on the peritoneal serosa. Microscopically, the pathognomonic characteristics that plead for the diagnosis of phlegmonous appendicitis are highlighted, and those accompany and strengthen the structural characteristics seen macroscopically on the operative parts. Morpho-pathologically acute phlegmonous appendicitis presents parietal microabscesses that can converge and open to the lumen. By perforating the appendix, the peritoneum (the thin membrane that lines the abdomen inside) becomes infected with bacteria, thus producing peritonitis. Peritonitis is a serious, life– threatening complication. This is a serious condition that requires urgent attention. Most often, the doctor can diagnose acute appendicitis based on the symptoms (presented above), the medical history and the physical examination of the patient. However, medical personnel may be needed to conduct further diagnosis and investigations, such as blood and urine tests, ultrasound, radiology, or magnetic resonance imaging (MRI). These investigations are necessary to help to guide the diagnosis, implicitly to differentiate from other conditions with similar symptoms.
Conclusions
It is important to clarify the misunderstood epidemiological features of appendicitis.
Perforating and non-perforating appendicitis appear to be separate entities, and as the need to spontaneously resolve appendicitis is essential having better reference materials to enable medical staff to make the correct decision is essential; this paper seeks to add to this area of knowledge. Ensuring that the diagnosis is correct can have important implications for the management of appendicitis suspicion. This must be supplemented with histological; assessments together with important personal, heredocolateral antecedents in the patient's pathological history. For example, determining the lymphocytopenia and neutrophil-lymphocyte ratio can predict bacteremia better than conventional infection markers in an emergency care unit. The histopathological stain remains important for such determinations.
Innovations and breakthroughs
The authors strongly emphasize and recommend that all appendectomy specimens be examined by histopathological analysis, even if the specimens have a normally coarse appearance.
References
- Rothrock, S.G., & Pagane, J. (2000). Acute appendicitis in children: emergency department diagnosis and management. Ann Emerg Med., 36; 39–51.
- Teo, a.t. et al. (2015). Institutional review of patients presenting with suspected appendicitis. anz J Surg., 85 (6); 420–424.
- Kaminski, A., Liu, I.L., Applebaum, H., Lee, S.L., & Haigh, P.I. (2005). Routine interval appendectomy is not justified after initial nonoperative treatment of acute appendicitis. Arch Surg., 140; 897–901. https://doi.org/10.1001/archsurg.140.9.897.
- Kotagal, M., Richards, M.K., Flum, D.R., Acierno, S.P., Weinsheimer, R.L., & Goldin, A.B. (2015). Use and accuracy of diagnostic imaging in the evaluation of pediatric appendicitis. Journal of pediatric surgery, 50(4), 642–646.
- Salö, M., Friman, G., Stenström, P., Ohlsson, B., & Arnbjörnsson, E. (2014). Appendicitis in children: evaluation of the pediatric appendicitis score in younger and older children. Surgery research and practice, 2014, 438076.
- Hale, D.A., Molloy, M., Pearl, R.H., Schutt, D.C., Jaques, D.P. (1997). Appendectomy: a contemporary appraisal. Ann Surg, 225; 252–261.
- Glass, C.C., & Rangel, S.J. (2016). Overview and diagnosis of acute appendicitis in children. Seminars in pediatric surgery, 25(4); 198–203.
- Rubér, M., Berg, A., Ekerfelt, C., Olaison, G., & Andersson, R.E. (2006). Different cytokine profiles in patients with a history of gangrenous or phlegmonous appendicitis. Clinical and experimental immunology, 143(1), 117–124.
- Blakely, M.L., Williams, R., Dassinger, M.S., Eubanks, J.W., 3rd, Fischer, P., & Huang, E.Y., et al. (2011). Early vs interval appendectomy for children with perforated appendicitis. Archives of surgery (Chicago, Ill. : 1960), 146(6), 660–665.
- Stewart, B., Khanduri, P., McCord, C., Ohene-Yeboah, M., Uranues, S., Vega Rivera, F., & Mock, C. (2014). Global disease burden of conditions requiring emergency surgery. The British journal of surgery, 101(1), e9–e22.
- Flum, d.r. (2015). Clinical practice. Acute appendicitis–appendectomy or the “antibiotics first” strategy. The New England journal of medicine, 372(20), 1937–1943.
- Fallon, S.C., Kim, M.E., Hallmark, C.A., Carpenter, J.L., Eldin, K.W., & Lopez, M.E., et al. (2015). Correlating surgical and pathological diagnoses in pediatric appendicitis. Journal of pediatric surgery, 50(4), 638–641.
- d'souza, N., & Nugent, K. (2016). Appendicitis. American family physician, 93(2), 142–143.
- Yang, H.R., Wang, Y.C., Chung, P.K., Chen, W.K., Jeng, L.B., & Chen, R.J. (2006). Laboratory tests in patients with acute appendicitis. anz journal of surgery, 76(1-2), 71–74. https://doi.org/10.1111/j.1445-2197.2006.03645.x
- Romano, A., Parikh, P., Byers, P., & Namias, N. (2014). Simple acute appendicitis versus non-perforated gangrenous appendicitis: is there a difference in the rate of post-operative infectious complications. Surgery Infection, 15; 517–520.
- Stahlfeld, K., Hower, J., Homitsky, S., & Madden, J. (2007). Is acute appendicitis a surgical emergency? The American surgeon, 73(6), 626–630.
- Andersson, R.E., Hugander, A.P., Ghazi, S.H., Ravn, H., Offenbartl, S.K., Nystrom, P.O., & Olaison, G.P. (1999). Diagnostic value of disease history, clinical presentation, and inflammatory parameters of appendicitis. World J Surg., 23; 133–140. https://doi.org/10.1007/PL00013174
- Friedell, M.L., & Perez-Izquierdo, M. (2000). Is there a role for interval appendectomy in the management of acute appendicitis? Am Surg., 66; 1158–1162.
- Pham, X.B.D., Sullins, V.F., Kim, D.Y., Blake, R., Kaji, A.H., de Virgilio, C.M., & et al. (2016). Factors predictive of complicated appendicitis in children. J Surg Res., 206; 62–66. https://doi.org/10.1016/pmid:27916376
- Samuel M. (2002). Pediatric appendicitis score. Journal of pediatric surgery, 37(6), 877–881. https://doi.org/10.1053/ jpsu.2002.32893.
- Mason r.j. (2008). Surgery for appendicitis: is it necessary? Surgical infections, 9(4), 481–488. https://doi.org/10.1089/ sur.2007.079
- Carr n.j. (2000). The pathology of acute appendicitis. Annals of diagnostic pathology, 4(1), 46–58. https://doi.org/10.1016/ s1092-9134(00)90011-x
- Yeh, C.C., Wu, S.C., Liao, C.C., Su, L.T., Hsieh, C.H., & Li, T.C. (2011). Laparoscopic appendectomy for acute appendicitis is more favorable for patients with comorbidities, the elderly, and those with complicated appendicitis: a nationwide population-based study. Surgical endoscopy, 25(9), 2932–2942. https://doi.org/10.1007/s00464-011-1645-x
- Kulik, D.M., Uleryk, E.M., & Maguire, J.L. (2013). Does this child have appendicitis? A systematic review of clinical prediction rules for children with acute abdominal pain. Journal of clinical epidemiology, 66(1), 95–104. https://doi.org/10.1016/j.jclinepi.2012.09.004
- Kwan, K.Y., & Nager, A.L. (2010). Diagnosing pediatric appendicitis: usefulness of laboratory markers. The American journal of emergency medicine, 28(9), 1009–1015. https://doi.org/10.1016/j.ajem.2009.06.004