Introduction
Mesothelioma is a rare neoplasm of serosal surfaces (such as pleura, peritoneum, pericardium and others) [1]. The most common form of these neoplasms is malignant pleural mesothelioma, peritoneal and pericardium mesotheliomas occur tenfold rarer, and mesotheliomas of other localizations are the most uncommon. The median latency of the disease is 32 years but it may range from 5 to 70 years.
Overseas annually hundreds of articles on mesothelioma are published, especially in context of occasional mesotheliogenic potency of asbestos.* To our knowledge the first article on this issue was published in 1933. In 40–50s of the XXth century single papers on this issue were published. In 1960 the results of J.Wagner’s study on association between mesotheliomas and exposure to crocidolite asbestos, were published, and later this study was recognized as classical [1]. From 70s of the XXth in western countries the most common etiological factor of mesothelioma was an inhalation of asbestos dust, primarily of amphibole asbestos (especially tremolite asbestos), that play a major role in causing the disease [2].
Not denying the role of amphibole asbestos in causing mesothelioma, a number of authors are skeptical about mesotheliogenic potency of chrysotile asbestos [3, 4]. Recent reports more often indicate that mesotheliomas may occur after exposure to other chemical (man-made mineral fibres, 9.10-dimethyl-1.2benzaanthracene, nickel, beryllium, mineralex, lead, polyurethane, ethylene oxide), physical (radioactivity), biological (Friend's virus (MC 29) and SV40) and many other carcinogenic agents [2–4].
Background incidence of mesothelioma is 1–2 cases per 1 million per year. In different countries incidence of mesothelioma varies widely from 0.15 to 29.01 cases per 1 million per year [1]. Mesothelioma incidence rates have been increasing throughout the industrialized countries in Western Europe, USA, Australia traditionally oriented to predominant use of amphiboles. The incidence in these countries varies from 4.33 in South Africa to 29.01 cases per 1 million per year in Belgium, at the average 8.06 cases as in USA. Mesothe* Asbestos is generic commercial name for a naturally occurring group of six different mineral fibers that differ in mineralogical structure, physicochemical properties and biological aggressivity and are uniform only on fibre structure. As these groups differ from each other on important features, which play the main role for its use, the types of asbestos are classified into two groups: serpentine and amphiboles. Serpentine includes magnesium silicate – chrysotile asbestos (white asbestos). The second group includes iron silicates, are known as amphiboles (actinolite, amosite (brown asbestos), anthophyllite, crocidolite (blue asbestos) and tremolite) [4].
lioma incidence rates in countries traditionally using chrysotile varies from 0.15 (Ecuador) to 4.81 per 1 million per year in Latvia, at the average 1.51 — for instance, in Estonia.
Incidence of mesothelioma in Russia is unknown [5]. In Russia a national register of mesothelioma doesn’t exist, and because of its’ rarity mesotheliomas haven’t been emphasized in official oncological statistics. Only in 1994 in St. Petersburg population cancer register mesotheliomas were classified as individual group of malignant neoplasms.
During the XXth century in Russia only 4 epidemiological studies of mesothelioma were conducted: local studies in Asbest [6] and Yekaterinburg [7], and two regional studies in the Republic of Karelia [8] and a pilot study in Sverdlovsk region [9]. The studies show that only in 12.0–29.4 % of cases an occupational exposure to asbestos may cause of mesothelioma [7–9].
So, currently we haven’t got reliable data on epidemiology of the mesothelioma in Russia and role of occupational factors, particularly asbestos, for developing this neoplasm. For clarification of range of statements on this issue we conducted comprehensive epidemiological analysis of mesothelioma in Sverdlovsk region, one of the most industrial administrative territories in Russian Federation.
The population of Sverdlovsk region is more than 4.5 million people, about 4.6 thousands of enterprises are situated here where about 2.1 million people are employed and more than 550 thousands from them work in harmful and dangerous conditions, and more than 100 thousands of people are exposed to substances, products, industrial processes and factors with proved carcinogenic potency and likely cancerogenic for the man [10].
In this region the largest deposit of chrysotile asbestos in the world named Bazhenovskoye, which is characterized by absolute absence of contamination with tremolite asbestos, is situated. The deposit is a part of eastern gabbro peridotite pack in Middle Ural, which also includes Alapayevskoye, Ostaninskoye and Rezhevskoye deposits of chrysotile asbestos. In the region there are 4 leading enterprises on asbestos production and field technological institute. In Sverdlovsk region more than 15000 of workers occupationally contact with chrysotile. Moreover situated in the region Sysert district is high in anthophyllite asbestos (Sysert region), there are 29 industrially significant deposits of anthophyllite and deposits of other amphiboles, development of which has been ceased.
Materials and Methods
As primary data we used official records of Sverdlovsk regional oncologic dispensary on new-onset diseases with clinicoradiologic diagnosis of mesothelioma for the period from 1981 to 2004. In all cases included into the study the diagnoses were confirmed using standard pathomorphological studies, and reexamination of histologic specimens was carried out. The data on population size in different areas and in Sverdlovsk region as a whole were obtained in regional statistical department.
Collected data were processed using recommended descriptive and cross epidemiological research methods. Incidence of mesothelioma was calculated per 1 million per year and was standardized by direct method, both for the region as a whole and for every municipal unit where they were revealed.
For all patients included into analysis it were studied occupational history personally or through relatives, and paraoccupational and environmental exposures to asbestos using special questionnaire developed by the group of international experts, for identifying potential asbestos exposure. Findings were specified in personnel department of enterprises where the patients with mesothelioma worked.
For all patients with occupational exposure to asbestos the value of total dust load on full weight of dust, received for the whole period of work activity was calculated.
Results
For 24 years (from 1981 to 2004) 226 diseases with primary clinicoradiologic diagnosis mesothelioma were registered in Sverdlovsk region. In 125 (55.3 %) cases the primary diagnosis was confirmed after morphological re-examination, and 101 (44.7 %) cases were excluded from the study because the primary diagnosis mesothelioma was proved incorrect. In addition 24 cases of lung cancer with pleural lesion, 19 cases of metastases of other cancers, 12 cases of pleuritis of nonneoplastic etiology and one case of complicated pancreatitis were revealed. In 14 cases intravital and postmortal morphological verifications were not carried out, in 28 cases primary materials were lost and 3 patients were inhabitant of other regions.
From 125 verified mesotheliomas 116 (92.8 %) cases were pleural mesotheliomas, 7 (5.6 %) were peritoneal mesotheliomas and 2 (1.6 %) were pericardial mesotheliomas. In 112 (89.6 %) patients malignant neoplasmes were revealed (including extrapleural) and in 13 (10.4 %) patients benign types of «mesothelioma» were revealed. By term «benign mesothelioma» we nominally mean localized mainly fibrous neoplasmes of pleura. Among malignant mesotheliomas on histologic type tumors of epithelioid type (72.9 %) prevailed, less often there were mesotheliomas of sarcomatous (13.6 %) and biphase (10.2 %) types.
The age of patients (67 men and 58 women) varied from 12 to 70 years, at an average 55.9±1.0 years, % of patients were productive Age and sexual differences at the diagnosis in cases of malignant and benign types of neoplasmes of different localizations and lesion area were not statistically significant.
Unless one case of pleural mesothelioma revealed during autopsy the lifetime of patients from the diagnosis of malignant mesothelioma ranged from 10 days to 1.10 years, at an average 7.1±0.8 months which is equivalent of results mentioned by Russian and foreign publications [1].
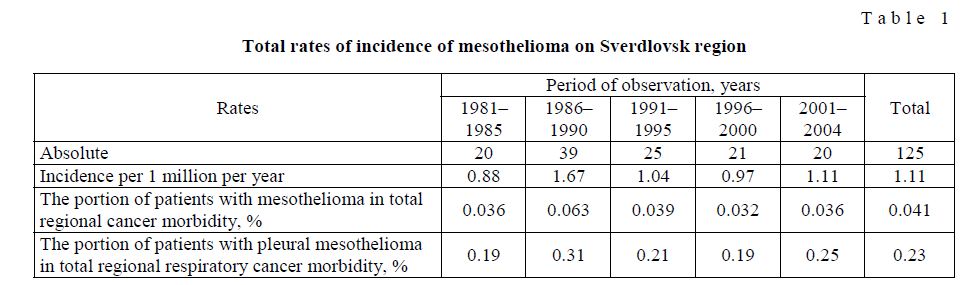
The interactive study of incidence of mesothelioma showed that despite of some increased incidence in 1985–1990 in the region the tendency to stabilization and even decrease is observed (Table 1).
Total rates of incidence of mesothelioma on Sverdlovsk region
T a b l e 1
Mesotheliomas were revealed in 32 from 55 municipal units of Sverdlovsk region. The bulk of neoplasmes was diagnosed in municipal unit Yekaterinburg — 50 cases (40.0 %), Asbest — 12 cases (9.6 %), Serov and Pervouralsk — 7 cases (5.6 %) and Kamensk-Uralsky — 6 cases (4.8 %) (Figure).
The incidence varied from 0.2 (Nizhny Tagil) to 27.1 cases per 1 million per year (Novoasbest), at an average 1.1 cases per 1 million per year for the period of study. In 16 (50 %) municipal units and in the region as a whole an average incidence of mesothelioma is agreed with global background level, i.e. 1–2 cases per 1 million per year.
In areas with enterprises on mining and manufacture of asbestos the incidence varied from 4.3 (Asbest — mining of chrysotile) to 27.1 cases per 1 million per year (Novoasbest — mining of crocidolite), and in Sysert antophillit province the incidence was 7.1 cases per 1 million per year. In towns Sukhoy Log and Beloyarsky, where enterprises «Sukholozhskasbocement» and «Beloyarskaya factory on asbestos board production» (which use chrysotile asbestos) are situated, mesotheliomas were not revealed.
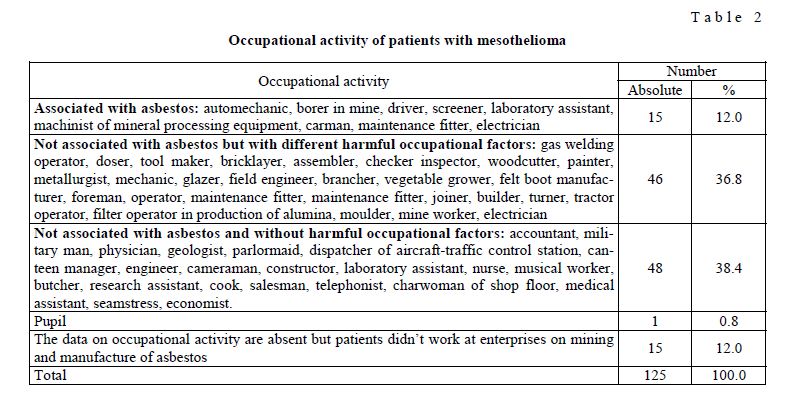
Occupational exposure to asbestos was revealed only in 15 (12.0 %) patients (Table 2). During labour activity 11 (8.8 %) patients occupationally contacted with chrysotile asbestos and 4 (3.2 %) patients — with amphiboles, including 3 patients contacting with crocidolite and one patient contacting with tremoilite. 7 from 15 patients worked at «Uralasbest», JSC (chrysotile), three patients — at mining and concentration complex Anatolyevsky (crocidolite) and three patients — at different motor transport enterprises in Yekaterinburg (chrysotile). One patient worked at talc plant Shabrovsky (tremolite) and one patients worked at «UralATI», JSC (chrysotile).
The age of patients with occupational exposure to asbestos varied from 37 to 75 years, at an average 55.7±2.6 years and was equal to corresponding figures for all patients with mesothelioma (55.9±.0 years). The age of patients at the first contact with asbestos varied from 18 to 27 years, at an average 21.5±1.1 years; and work experience varied from 3 months to 45 years, at an average 21.3±3.2 years. Mesotheliomas developed during 13–68 years after beginning of exposure, at an average — after 33.9±3.8 years. It is important to note that occupational activity of patients with occupational exposure to asbestos in all cases was in conditions of high levels of exposure, which were common to 50–60s years of the XXth century [11].
The labor activity of patients not associated with asbestos was presented by wide range of occupations, including 46 workers (36.8 %), 17 technologists (13.6 %), 13 clerks (10.4 %), 9 medicine workers (7.2 %) and 7 scientific workers (5.6 %). In 15 patients (12.0 %) the area of working activity wasn’t revealed but at they didn’t work at enterprises on mining, processing and manufacture of asbestos on Sverdlovsk region. In one case (0.8 %) the patient with malignant mesothelioma was 12-years-old boy.
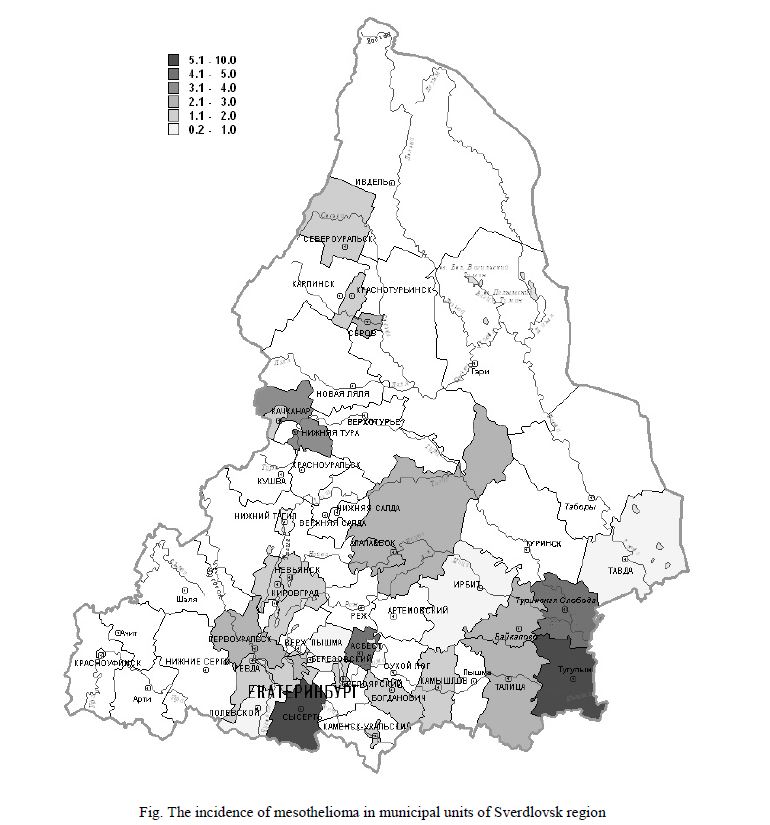
Fig. The incidence of mesothelioma in municipal units of Sverdlovsk region
Among nonprofessional occupations during labour activity not associated with asbestos but with different harmful factors the most patients with mesothelioma occupationally contacted with substances, products, industrial processes and factors, potentially causative for mesothelioma: nickel, chrome, smut, man-made mineral fibres, and radiological agents.
Differences in age, sex and localization at the diagnosis in cases occupational malignant and benign mesotheliomas were not statistically significant.
Life expectancy of patients with occupational exposure to chrysotile asbestos from the diagnosis of malignant mesothelioma was 5.4±1.3 months; and for amphiboles — 6.5±2.2 months, and in both cases this figure was statistically significantly lower (р<0.01) than for patients without exposure to asbestos.
Some features of development of malignant mesothelioma in patients with occupational exposure to different types of asbestos are shown in the Table 3.
Occupational activity of patients with mesothelioma
T a b l e 2
Some data of occupational history in patients with malignant mesothelioma with exposure to asbestos, M±m (variations)
T a b l e 3
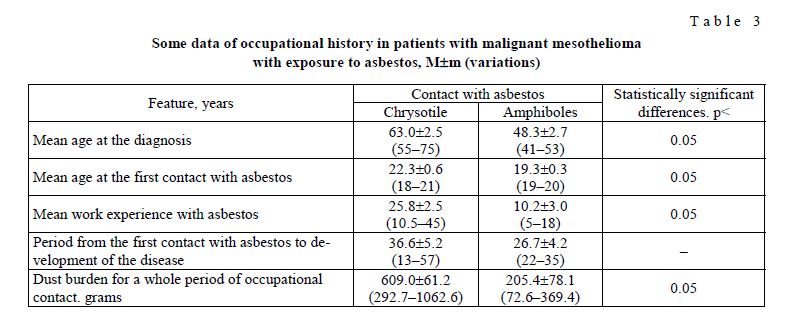
As the table 3 suggests in the group of patients with the exposure to amphibole asbestos mesotheliomas statistically significantly (р<0.05) developed in earlier age, with less work experience and virtually in 3 times lower dust load, than in the group of patients with exposure to chrysotile asbestos. Malignant neoplasms also were diagnosed after shorter time from the first contact with asbestos, but in that case the differences were not statistically significant.
Conclusions
- The first Russian integrated epidemiological study of mesothelioma in Sverdlovsk region showed that an average incidence of mesothelioma is agreed with global background level, e. 1–2 cases per 1 million per year.
- Asbestos, particularly, chrysotile is not a leading, and moreover obligate causative factor for development of the disease. The disease has got pluricausal
References
- Wagner C., Sleggs C.A., Marchand P. Diffuse pleural mesothelioma and asbestos exposure in the Northwestern Cape Province // British journal of industrial medicine. — 1960. — Vol. 17. — № 4. — P. 260–271.
- Malignant mesothelioma: advances in pathogenesis, diagnosis, and translational therapies / Edited by Pass H.I., Vogelzang , Carbone M. — Springer: New York, 2005. — 854 p.
- Chrysotile asbestos: Environmental Health Criteria 203. — World Health Organization. — Geneva, 1998. — P. 106–128.
- Asbestos and other natural mineral fibres: Environmental Health Criteria 53. — World Health Organization. — Geneva, — P. 11.
- Bianchi , Brollo A. et al. Malignant mesothelioma in Central and Eastern Europe // Acta Medicina of Croatia. — 2000. — Vol. 53. — № 4–5. — P. 161–164.
- Kogan M., Berzin S.A. Incidence of pleural mesothelioma under impacts of chrysotile asbestos dust // Occupational hygiene and occupational diseases. — 1986. — № 9. — P. 9–12.
- Kashansky S.V., Tomilova N.E. et al. Mesothelioma incidence in Yekaterinburg (preliminary report) // Current problems of preventive medicine in Ural region: collection of scientific papers and scientific-practical work, dedicated to 80th anniversary of Russian sanitary and epidemiological service. — Yekaterinburg, 2002. — P. 139–143.
- Romanchuk Y. Impact of occupational exposure on cancer morbidity of inhabitants of republic of Karelia // Materials of the International seminar of working group on cooperation under the program «Asbestos», May 18–20, 1999, Petrozavodsk. — Petrozavodsk, 1999. — P. 13–23.
- Fedosenko N.E. Mesothelioma in Sverdlovsk region // Issues on cancer care facilities at the stage of reforming of public health service [collected works]. — Yekaterinburg, 1996. — P. 28–29.
- Shaburov P., Kashanskiy S.V., Kashanskaya E.P. Occupational oncopathology in Sverdlovsk region (preliminary results) // Current issues of preventive medicine, environment and public health in industrial regions in Russia: Collection of scientific papers, dedicated to 75th anniversary of foundation of Yekaterinburg medical research center for prophylaxis and health protection of industrial workers. — Yekaterinburg, 2004. — P. 414–421.
- Kashanskiy S.V., Scherbakov S.V., Kogan F.M. Dust levels in workplace air (a retrospective view of «Uralasbest») // Treatment and prevention of asbestos diseases: Volume 15 of the sourcebook on asbestos diseases: medical, preventive, and socioeconomic aspects. — Edit. Peters G.A. and Peters B.J. — LEXIS® Law Publishing, 1997. — P. 337–354.