Introduction
The problem of asbestos-related lung diseases remains urgent although many foreign and domestic studies, including hygienic, epidemiologic, and clinical X-ray studies, have been devoted to this issue.
Only chrysotile asbestos is produced and applied in Russia. Russia has a perspective source of raw chrysotile prepared of a long-term exploitation [1]. Over 40 thousand workers are exposed to asbestos dust.
The main industries with potential occupational exposures to asbestos dusts include asbestos mining and milling and the production of asbestos-containing products (asbestos-cement, asbestos technical and asbestos textile materials).
The main asbestos consumer today is the production of asbestos-cement products (corrugated and flat sheets, pipes, etc.) that are widely used in industrial and civil construction.
Other widely used asbestos-containing materials include asbestos-containing noise and heat insulation — molded products, friable covers (asbestos perlite, vermiculite, etc.) that are prepared in place by mixing asbestos with different fillers; asbestos board; asbestos-technical friction products — clutches, brake linings and pads, etc.; asbestos textile products — fabric, cords, gaskets and pads, etc. It is also possible to use asbestos in the product of asphalt, bituminous mixtures and many other materials and products.
The exposures to asbestos dust above the exposure limits can be observed at various types of activities related to installation, maintenance, alteration, and removal of asbestos-containing building materials, especially of low-density insulation in many industries (construction of industrial and civil objects, energetic, ferrous and non-ferrous metallurgy, glass industry, shipbuilding, etc.) [2]. This fact should be taken into consideration when planning and conducting pre-exposure and periodic preventive medical check-ups.
The main occupations with potential high exposures to chrysotile include asbestos miners and millers, insulation workers (including those involved in shipbuilding) and other builders who apply, repair or remove chrysotile-containing heat and noise-insulation materials. Exposures to high concentrations of chrysotile fibers are also possible in the manufacture of asbestos textiles, asbestos cement and asbestos technical products, during some operations, e.g. mixing of basic components, if the established safety measures are neglected [1].
The exposure to amphibole fibers that poses a much higher health risk for workers even at minimal levels compared to chrysotile fibers is possible during maintenance and repair of ships built abroad [1].
A long-term exposure to chrysotile dust above the exposure limits and even to minimal concentrations of amphiboles can increase the risk of asbestos-related bronchopulmonary diseases, transform clinical and Xray manifestations, the clinical course and outcomes of asbestos-related diseases. Distinctive features of the development and clinical course of asbestos-related diseases make it necessary to take preventive actions in order to eliminate them. The main direction of prevention of occupational asbestos-related lung diseases nowadays is the development of criteria of health disorders based on early and reversible changes preceding the manifestation of apparent clinical signs and syndromes in comparison with the total asbestos exposure [3]. The basis for medical prevention is the development of criteria of risk of lung diseases, early detection and timely rehabilitation in case of asbestos exposure [4]. Rehabilitation actions aimed at a complete health recovery in workers with primary disorders of various organs and systems [3, 5] and at preserving work potential should be based on rehabilitation medicine aimed at improving workers’ health and raising functional reserves.
With this goal in view we analyzed the results of an in-depth clinical, X-ray, laboratory, and functional examination and of hygienic studies of 771 persons with different asbestos-related diseases and signs of health disorders that can be related to asbestos exposures.
On the basis of obtained data we established the most significant criteria of effect of asbestos dusts on respiratory organs — from the initial signs of effect to the development of the pathologic process. This allowed us to substantiate and define three risk groups by the development of bronchopulmonary pathology in workers following the asbestos exposure:
- The first risk group includes workers at risk of bronchitis: patients complain of inconstant nonproductive cough, exercise dyspnea; at auscultation rough breathing is heard and a positive forced expiratory spirogram is sometimes noted, in some cases — the decrease in the rates of the respiratory function to Stage 1.
- The second risk group includes workers at risk of asbestosis: early diffuse changes in the lung parenchyma (profusion 0/1 and 1/0) are determined during the X-ray examination, peribronchial sclerosis in the middle and lower lung compartments, early isolated changes of the visceral pleura (interlobar, costal and diaphragmatic) and possible early restrictive impairment of the respiratory
- The third risk group includes individuals with presumable asbestosis (0–1): early diffuse lung fibrosis (profusion 1/1) is determined during the X-ray examination, without changes or with prevalent blurred lesions of the visceral pleura, isolated changes of the parietal pleura; patients complain of inconstant dry cough, exercise dyspnea, and early restrictive impairment of the respiratory
In order to develop systematic measures for prevention, medical rehabilitation and detection of early signs of exposure to asbestos dust we analyzed results of mass prophylactic examinations of 774 workers involved in asbestos mining, milling, and the production and use of asbestos-containing products. In accordance with the defined risk groups we took into account the frequency and prevalence of signs of effect of asbestos dust on respiratory organs of the workers, the number of diagnosed asbestos-related bronchopulmonary diseases among the examined workers of various production groups, and the analysis of asbestos dust concentrations at workplaces.
Individuals of the first and second risk groups by the development of bronchitis and chrysotile asbestosis are subject to case follow-up with an in-depth clinical examination. The risk group including individuals with presumable chrysotile asbestosis is the third group requiring the verification of X-ray changes in lungs in hospital environment.
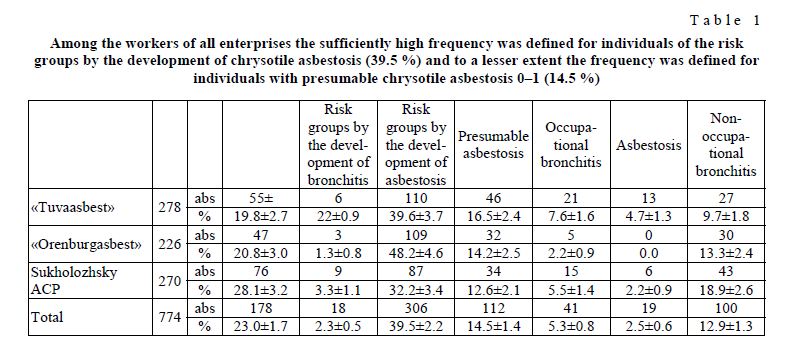
The analysis of results of mass prophylactic examinations of 774 workers involved in production (the Mining and Ore Dressing Companies «Tuvaasbest» and «Orenburgasbest», the Sukholozhsky Plant of Asbestos-Cement Products) by taking into account clinical functional and X-ray criteria specified by us for the development of bronchopulmonary pathology helped define the risk groups for the development of bronchitis and chrysotile asbestosis, presumable chrysotile asbestosis (0–1) and the groups with bronchopulmonary pathology: professional bronchitis and chrysotile asbestosis (Table 1).
The low frequency of workers of the risk group by the development of bronchitis (2.3 %) was noted among the examined workers of all enterprises. Professional bronchitis was diagnosed in 5.3 % of cases and definitely more often in workers of the «Tuvaasbest» Company (7.6 %) than in workers of the «Orenburgasbest» Company (2.2 %). Professional bronchitis was diagnosed in 5.5 % of the examined workers of the Sukholozhsky Plant of Asbestos-Cement Products. Chrysotile asbestosis was revealed in 2.5 % of the examined workers and it was revealed more often in workers of the «Tuvaasbest» Company (4.7 %) with high exposures to asbestos rock dust. Chrysotile asbestosis was revealed in 2.2 % of workers of the Sukholozhsky Plant of Asbestos-Cement Products and chrysotile asbestosis at the «Orenburgasbest» Company was not diagnosed at all.
T a b l e 1
Among the workers of all enterprises the sufficiently high frequency was defined for individuals of the risk groups by the development of chrysotile asbestosis (39.5 %) and to a lesser extent the frequency was defined for individuals with presumable chrysotile asbestosis 0–1 (14.5 %)
In order to reveal early signs of exposure to chrysotile-containing dust and take preventive actions all examined workers of the «Tuvaasbest» and «Orenburgasbest» Companies, the Sukholozhsky Plant of Asbestos-Cement Products were distributed by groups depending on the dust load value (DL) for all years of work (Table 2).
T a b l e 2
The number of workers with a different degree of risk for developing asbestos-related diseases depending on the dust lung load
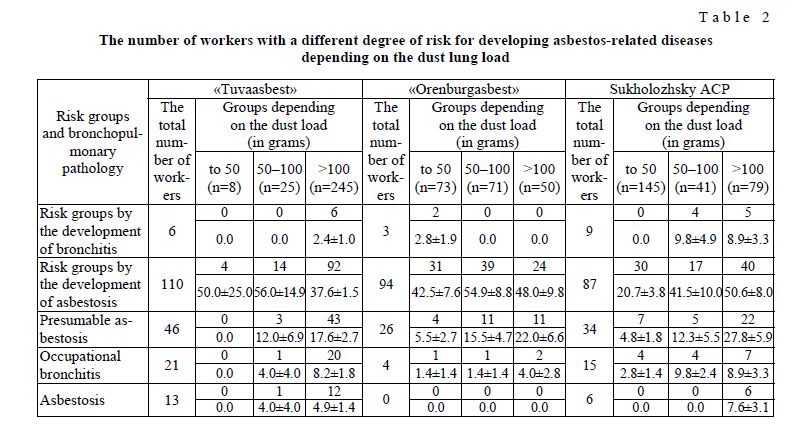
The analysis of clinical functional and X-ray data depending on the dust lung burden of asbestos miners and millers helped reveal a clear association between the frequency of some signs of asbestos exposure and the dust burden close to 50 grams, which became the critical exposure value for the development of asbestosrelated bronchopulmonary diseases. The obtained results give the opportunity to control the development of asbestos-related lung diseases and take timely medical and social measures for their prevention and rehabilitation.
The current system and principles of primary prevention, medical diagnosis and rehabilitation require the improvement of organizing medical and sanitary care for individuals exposed to asbestos.
Medical preventive measures should combine two main directions: conducting pre-exposure and periodic medical examinations in order to prevent the development of bronchopulmonary pathologies, defining groups of workers at risk of asbestos-related diseases, and prescribing preventive rehabilitation of workers at risk to restore the adaptive failure and preserve health.
The analysis of obtained data enables us to substantiate the main provisions and the plan of medical and social measures for prevention and rehabilitation of asbestos-related bronchopulmonary diseases from the position of clinical, X-ray, functional and hygienic criteria:
- Constant medical surveillance of workers exposed to asbestos dust during the employment and postexposure
- Timely formation of risk groups taking into account a complex effect of asbestos and other adverse occupational and environmental factors on
- Special attention to detection of early signs of health effects of asbestos not only in workers of asbestos mines, mills and the production of asbestos-containing materials but also of industries with potential asbestos exposures related to the uncontrolled use of asbestos-containing materials and
- Provision of personal recommendations for preserving and prolonging the ability to
- Provision of personal recommendations for taking preventive and rehabilitative
- Development of the database on workers’ health, starting with the pre-exposure medical examination, with the following accumulation and registration of all health disorders (including results of preventive medical examinations, admissions and results of check-ups) including occupational and somatic
- Based on accumulated data and systematization of results a health passport of each worker is created with the purpose of case follow-up.
- Application of standard documentation for the follow-up and registration with the evaluation of results of preventive medical examinations for timely definition of risk groups and taking preventive and rehabilitation actions aimed at preserving and improving
To improve and optimize medical preventive actions for early detection, treatment and rehabilitation of individuals exposed to asbestos, it is necessary to develop medical standards including the plan of medical surveillance of workers (during pre-exposure and periodic medical examinations) and cases of asbestosrelated diseases, basic therapy treatment and rehabilitation actions including specific recommendations for sanatorium and spa treatment.
Difficulties in diagnosis and differential diagnosis, in solving expert questions are primarily caused by insufficient equipment of medical units, Centers and departments of occupational pathology with modern Xray, laboratory, and functional instrumentation. It is also important to note insufficient preparation of occupational pathologists at postgraduate courses on issues of prevention, early detection, diagnosis, treatment, and rehabilitation of asbestos-related diseases.
Nowadays much attention is paid to prevention of asbestos exposure at workplaces and related health changes in the majority of chrysotile mines, mills and in the production of chrysotile-containing products. At the same time, it has been noted that in many industries (primarily in energetic and shipbuilding) insufficient attention is paid to those cases where the uncontrolled use of friable products may pose a real health risk to workers.
The issues of health protection of asbestos workers include training on prevention of respiratory diseases, including asbestos-related diseases. It covers comprehensive health-improving measures aimed at increasing resistance of the organism: healthy lifestyle (no smoking, no alcohol abuse, etc.), going in for sports, healthy nutrition, and timely treatment of colds.
Measures for prevention and elimination of asbestos-related diseases also include basic responsibilities/obligations of asbestos workers:
- workers employed by industries with potential asbestos exposures shall be trained beforehand in accordance with instructions of the enterprise on safety in the use of asbestos;
- according to the Order of the Ministry of Health and the Ministry of Industry of the Russian Federation of 14 March 1996 No. 90 workers employed by industries with potential asbestos exposures shall take a pre-exposure medical examination and regular medical examinations;
- within the limits of their responsibilities and work descriptions workers must contribute to control, prevention and minimization of asbestos concentrations in the work They must report about extraordinary conditions at workplaces and/or situations disrupting the production process;
- workers must periodically participate in educating and instructing programs on occupational safety;
- all workers exposed to asbestos must use personal protective equipment in accordance with typical and departmental standards supplied by the employer;
- workers with frequent colds and somatic diseases are liable to dispensary registration in medical units or local polyclinics because these illnesses may become risk factors of asbestos-related
Thus, the development of a national program for prevention and elimination of asbestos-related diseases is the most important socio-economic task that envisages integration and harmonization of all elements of medical and technical measures aimed at improving the quality of medical care for asbestos workers.
References
- Asbestos-related pathology: diagnosis, clinical picture, pathomorphology, prevention and rehabilitation: Handbook for Physi— M., 2008. — 67 р.
- Domnin S.G., Kashansky S.V. et al. Asbestos — modern problems of occupational medicine and environmental science // Prevention of asbestos-related diseases: Collected articles. — Asbestos, 2002. — P. 118–122.
- Izmerov F., Kovalevsky E.V. Fundamentals of developing of national program for elimination of diseases which depend on asbestos // Occupational Medicine: Implementing the Global Plan of Action for the health of workers in 2008–2017: Proceedings of the All-Russian conf. on the 85th anniversary of the Institute of Occupational Medicine, RAMS. — M., 2008. — P. 116– 118.
- Kovalevsky V. Assessment of natural and artificial mineral fiber particles in the air, non-production objects // Occupational Medicine and Industrial Ecology. — 2004. — № 1. — P. 10–16.
- Razumov N., Bobrovnitskii I.P., Shakulov A.V. Restorative medicine and its role in public health // Bulletin of the Scientific Board of «Medical and ecological problems of workers». — 2004. — № 3. — Р. 81–84.