The Directive of the European Union 1999/77/EU on the global asbestos ban is based on results of occupational studies and the assessment of risk of asbestos-related respiratory diseases (such as lung cancer, malignant pleural mesothelioma, etc.) in workers since such diseases develop only after 20–40 years from a long-term exposure to high concentrations of asbestos-containing aerosols. At the same time, the results of assessing risks of developing a respiratory malignancy from environmental exposures to low concentrations of chrysotile dust still remain the subject of debate.
A statistically significant increase in the incidence rates of lung cancer and malignant pleural mesothelioma was observed only in the population environmentally exposed to amphibole asbestos [1, 2]. Moreover, primary attention is paid to mesotheliogenic effects of asbestos. Meanwhile, the incidence rate of lung cancer in men is two to three orders of magnitude higher than that of pleural mesothelioma.
According to the data of the Ekaterinburg Medical Research Center for Prevention and Health Protection in Industrial Workers of Rospotrebnadzor the most significant sources of air pollution from the point of view of environmental hygiene are gross emissions from chrysotile mines and mills and fiber emissions from uncultivated tailing dumps, especially dusty ones [3]. We, therefore, conducted an epidemiologic study of respiratory malignancies in men residing in the town of Asbest, Sverdlovsk Region. This town has been chosen as the study object because it is located in the vicinity of the world largest Bazhenovskoye deposit of chrysotile asbestos that has been developed for over 125 years now. The urban population mostly suffers from para-occupational and environmental exposure to chrysotile.
As primary data we used official reports of the Sverdlovsk Regional Cancer Dispensary that contain information about all incident lung cancer cases among men registered in the town of Asbest and the Sverdlovsk Region during 51 years (1958–2008).
The occupational history of the male lung cancer cases in Asbest was established using archive data of the personnel departments of Uralasbest, JSC, UralATI, JSC, and other asbestos industries in Russia and CIS countries. All persons with the registered occupational contact with chrysotile asbestos lasting at least a year were considered occupationally exposed.
Information about the size of population and its sex and age composition was obtained from the Sverdlovsk Regional Statistical Office.
Based on the accumulated data we estimated intensive indicators of the incidence per 100 thousand of the total male population of Asbest, male population of Asbest never employed in the asbestos industry and of the Sverdlovsk Region as a whole. In order to eliminate age differences we performed a direct standardization taking the age-specific structure of the population of the Sverdlovsk Region based on census data for the appropriate year as a standard.
To have a clearer understanding of the dynamics of lung cancer incidence rates we compared 5-year averages. The analysis was performed in Microsoft Excel 1997–2003 and STATISTICA v 6.0.
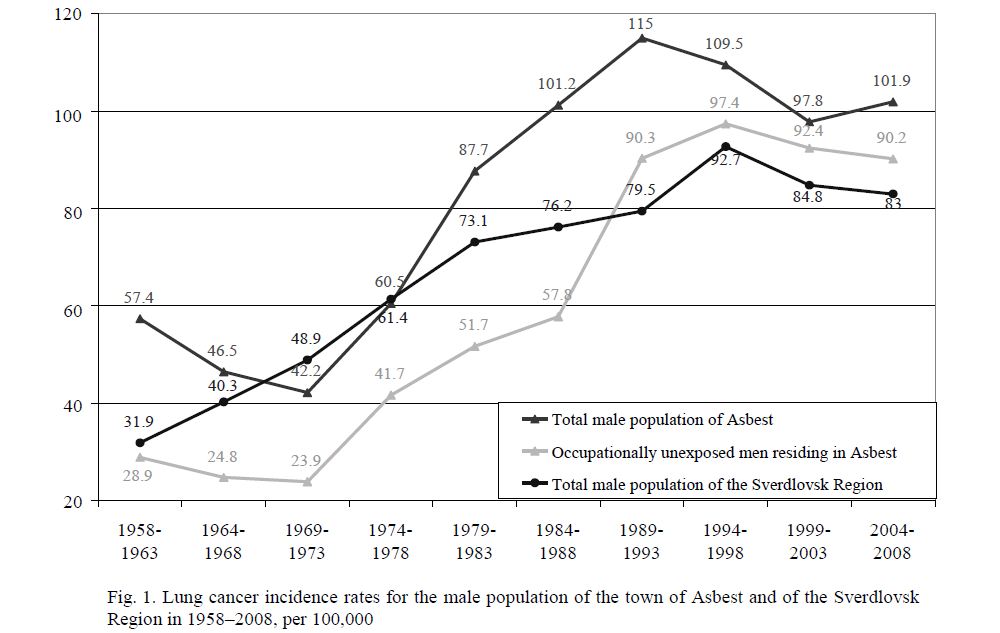
Fig. 1. Lung cancer incidence rates for the male population of the town of Asbest and of the Sverdlovsk Region in 1958–2008, per 100,000
Due to huge emissions of Uralasbest mills in 1930–1940s average airborne dust concentrations in the residential area of Asbest exceeded the then current maximum permissible concentration of 0.5 mg/m3 by tens and hundreds of times.
A fundamental improvement of the situation was first noted in the town in late 1950s when old factories constructed in the residential area in the end of the 19th and the first part of the 20th century were demolished and new, hygienically and technologically advanced and powerful factories built outside the residential area and having proper sanitary zones were put into operation; at the same time, the existing factories and mills were equipped with effective electric and hose filters. In 1969 the centralized system of pneumatic transport and aspiration with efficiency to purify the contaminated air in hose filters equaling 99.9–99.999 % was installed in Mill No. 6 for the first time in Russia. As a result of this improvement total ambient emissions of asbestos dust dropped from 200 tons per day in 1960 to 5.8 in 2008 (by 34.5 times).
A dramatic improvement of ambient air quality indices was registered in 1994 when Mill No. 5, the last mill located in the residential area of the town, was closed. Complex measures for reduction of industrial emissions in ambient air taken at Uralasbest, JSC led to a significant decrease in ambient air pollution with asbestos dust in late 1990s to concentrations of 0.15–0.17 mg/m3 and with chrysotile fibers — to 0.02 f/ml,
i.e. to the level and below hygienic standards equaling 0.15 mg/m3 and 0.06 f/ml, respectively.
During that period areal distribution of asbestos dust including chrysotile fibers was uniform across the whole residential area of the town. Average monthly concentrations in samples taken at stationary monitoring sites at distances of 1.0, 2.0, and 2.5 km from the open pit were almost similar. In some daily average samples we found a slight excess of the maximum permissible concentration of asbestos dust but the percentage of such samples was only 15–20 %.
The study of lung cancer incidence in men living in Asbest, both occupationally and environmentally exposed to chrysotile asbestos, showed that not a single case of lung cancer had been registered in the age group under 30.
We found no statistically significant differences in the age structure of lung cancer cases among men residing in Asbest, both occupationally and environmentally exposed to chrysotile, and in the Sverdlovsk Region as a whole. The highest incidence rates (37.0–38.5 %) in all exposure groups were registered in the age group of 60–69 years.
A comparative study of lung cancer incidence rates for men in Asbest and the Sverdlovsk Region showed that in different intervals of this period they varied in a wide range (Fig. 1). During 10 years, 1958– 1967, the incidence rate for the total male population of Asbest was 1.3 times higher than that in the Sverdlovsk Region (46.0 vs. 35,2 ‰ on the average for the period). In the following 11 years (1967–1977) the picture changed to the opposite: the incidence rate in Asbest dropped and became 1.2 times lower than that in the Region (41.4 against 50.8 ‰). Only in 1973 the incidence rate in Asbest was 1.4 times higher than that in the region (70.4 vs. 51.2 ‰). During the period of 1958–1977 all differences were not statistically significant. From 1978 the lung cancer incidence rate for the total male population of Asbest exceeded the regional average: by 1.3 times in 1980–1999, by 1.2 times in 2000–2008, but only in 1984–1988 and in 2004–2008 it was significantly higher than the regional average (p<0.05).
For the whole observation period the percentage of occupationally exposed men from the total lung cancer incident cases in Asbest dropped from 49.6 % in 1960s to 9.0 % in the beginning of the 21st century (R2 = 0.766).
The analysis of characteristics of the lung cancer incidence rate for occupationally unexposed male residents of Asbest after exclusion of the exposure group showed that during 31 years, 1958–1988, it was significantly 1.1–2.0 times lower than the regional average (р<0.05). Since 1989 the incidence rate in this group has been 1.1 times higher than the regional average one but this difference is not significant.
Having compared lung cancer incidence rates for the male population of Asbest to emissions of Uralasbest, JSC and airborne dust concentrations in the town we found that only during 15 years, 1958– 1973, these indicators decreased simultaneously (Fig. 2). In 1973–1989, despite a continuous improvement of environmental conditions in the town, the lung cancer incidence rate in the male population of Asbest increased steadily.
Since 1989 a sustained decline in the lung cancer incidence rate for men by 4.8–10.7 % every 5 years has been registered in Asbest. A similar decrease in the lung cancer incidence rate in the Sverdlovsk Region and among the unexposed male population of Asbest has been observed since 1994 by 2.1–8.5 % and 2.4– 5.1 %, respectively.
Thus, the reduction in gross emissions of Uralasbest, JSC resulted in a dramatic improvement of environmental conditions in Asbest that, in its turn, after 30 years led to a registered in the past 20 years sustained decline in lung cancer incidence rates for men.
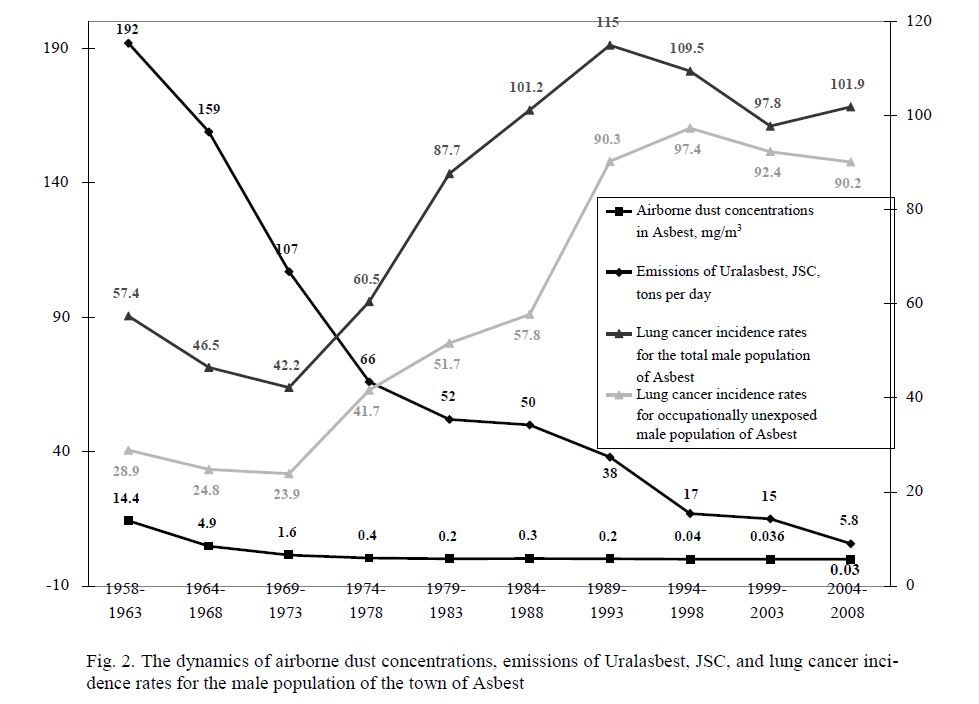
Fig. 2. The dynamics of airborne dust concentrations, emissions of Uralasbest, JSC, and lung cancer incidence rates for the male population of the town of Asbest
These epidemiologic studies have also demonstrated that the observed lung cancer incidence rate for men in Asbest appeared to be 44 % lower than the predicted value [4]. This finding is yet another evidence of greater reliability of epidemiologic studies compared to modeling that has a large number of uncertain variables.
References
- Malignant mesothelioma: advances in pathogenesis, diagnosis, and translational therapies / Pass H., Vogelzang N., Carbone (eds.). — Springer: New York, 2005. — 854 p.
- Pathology of asbestos-associated diseases / Roggli L., Oury T.D., Sporn T.A. (eds.). — Springer: New York, 2004. — 421 p.
- Plotko G., Selyankina K.P. et al. Hygienic issues of environmental protection and public health in the areas of chrysotile asbestos production and use // Hygiene and Sanitation. — 2005. — № 6. — Р. 70–71.
- Berzin A., Kogan F.M., Vasyov R.V. Lung cancer incidence rates in the town of Asbest, Sverdlovsk Region, in 1958–1997 // Ural Medical Review. — 2000. — № 3–4. — Р. 55–57.